Muscles(musculi) They represent the active part of the musculoskeletal system and provide movements that are of paramount importance for human life. Muscles are formed striated (striated) muscle tissue, component skeletal muscles. The muscles of internal organs and blood vessels consist of non-striated (smooth) muscle fibers.
DEVELOPMENT OF MUSCLES AND FASCIA
Skeletal muscles develop from the dorsal part of the middle germ layer, located on the sides of the notochord and neural tube. The dorsal section of the mesoderm at the end of the 3rd week of embryonic development begins to divide into primary segments, or somites. The division of somites occurs gradually from the cranial to caudal regions. By the 6th week, the embryo has 39 pairs of somites: 4 occipital, 8 cervical, 12 breast, 5 lumbar, 5 sacral and 5 coccygeal Somites are separated from each other by transverse connective tissue septa, or myoseptami. Subsequently, as the embryo develops, the somites are divided into 3 parts: dorsomedial - myotome, from which skeletal muscles are formed; ventrolateral - dermatome, forming the connective tissue basis of the skin; the remaining part of the somites forms sclerotome, the cells of which subsequently differentiate into vertebrae (Fig. 47). The myotome, growing in the anterior direction, is divided into dorsal and ventral parts. The dorsal part forms the back muscles, and the ventral part forms the muscles located on the front and lateral surfaces of the body. Muscle development is closely related to the evolution of the nervous system. Branches of spinal nerves, formed at the same segmental level according to the division of the myotome, grow into each myotome. The spinal nerves are divided into anterior and posterior branches.
Rice. 47. Cross section through the body of a vertebrate embryo: 1 - r. ventralis n. spinalis; 2 - r. dorsalis n. spinalis; 3 - chorda dorsalis; 4 - limb bud; 5 - ventral process of mesoderm; 6 - intestine; 7 - visceral leaf of the lateral plate; 8 - parietal leaf of the lateral plate; 9 - body cavity; 10 - primary segments (somites); 11 - ectoderm; 12 - spinal tube; 13 - dermatome; 14 - myotome; 15 - sclerotome; 16 - nephrotom
The muscles of the head and neck develop from the mesoderm of the gill arches and are called branchiomeres. From the mesenchyme of the first arch, the masticatory muscles, part of the neck muscles, and also the tensor tympani muscle are formed. These muscles are innervated by motor fibers of the trigeminal nerve.
The facial (facial) muscles are formed from the second branchial arch by migration from the neck to the face and head, and along with the muscle mass of the hyoid arch, the branches of the facial nerve are also transferred. From the third branchial arch the stylopharyngeal muscle and part of the pharyngeal constrictors, innervated by the IX pair of cranial nerves, are formed. The muscles lying below the hyoid bone and the deep muscles of the neck originate from the cervical myotomes. They are innervated by branches from the cervical plexus. From the fourth branchial arch the muscles of the larynx and the remaining constrictors of the pharynx, innervated by the X pair of cranial nerves, develop.
Further development of the muscular system occurs in various ways. Longitudinal splitting of muscle mass leads to the formation of separate independent muscles. This is how the trapezius and sternocleidomastoid muscles are formed. Tangential splitting promotes the formation of two oblique and transverse muscles of the anterolateral abdominal wall. Fusion of parts of adjacent myotomes can lead to the formation of a single muscle. For example, the rectus abdominis muscle is formed as a result of the fusion of the anterior parts of the VI-VII thoracic myotomes. Sometimes partial or complete migration of muscle primordia to other segmental levels is observed: for example, facial muscles migrate to the face from the neck area. Degeneration of the entire muscle segment or part of it is possible, followed by replacement by connective tissue and the formation of aponeuroses. For example, a tendon helmet of the head is formed, connecting the 2 bellies of the occipitofrontal muscle. Muscles that remain in the same place during development form local, autochthonous, muscles (autos- the same, chton- Earth). These include the rectus abdominis muscle. Muscles that move from the trunk to the limbs are called trancofugal (truncus- trunk, fugo- put to flight): for example, the serratus anterior muscle, and the muscles moving from the limbs to the torso - truncopetal (peto- I strive). The latter includes, for example, the pectoralis major muscle.
GENERAL MYOLOGY
The main function of both striated and non-striated muscle tissue is contractility. Skeletal muscle tissue consists of muscle fibers 4-5, less often 10-12 cm long. Each muscle fiber has a sheath - sarcolemma, under which there are many cores. Beneath it is located sarcoplasm containing contractile filaments - myofibrils. Under a microscope, the transverse striations of the muscle fibers are visible. The heterogeneity of the structure of the fibers of skeletal muscle tissue is due to the fact that myofibrils consist of light (isotropic, band I) and dark (anisotropic, band A) stripes. Skeletal muscle makes up about 1/3 of an adult's body weight and about 1/4 of a child's body weight. As you age, muscle mass decreases. In athletes, muscle mass can account for 50% of total body mass.
Humans have more than 400 skeletal muscles. The shape of the muscles is varied (Fig. 48). Muscle classification is presented in Table 1.

Rice. 48. Muscles of various shapes:
I - fusiform; II - single-pinnate; III - bipinnate; IV - two-headed; V - muscle with tendon jumpers; VI - digastric; VII - sphincter (circular)
Table 1. Muscle division

The muscles on the torso are often flat. The muscles of the limbs, on the contrary, are fusiform or feathery, with a smaller area of attachment to the bones. They usually participate in movements with a pronounced amplitude. Movements caused by short muscles have a small range. Unlike long muscles, short ones usually have greater strength and can overcome significant resistance.
In the long muscles there is a middle thickened part - the abdomen (venter), passing into tendons at the ends (tendo), by which the muscle is attached to the bone. In this regard, a distinction is made between the tendon of origin and the tendon of insertion, muscles corresponding to two points of connection with the bones: fixed And mobile. The tendon of the beginning together with part of the belly of the muscle is called the head (caput). Muscles can also be attached to bones by short fibrous bands associated with intramuscular connective tissue. This attachment is called fleshy and is most often observed at the origin of the muscle. There are also heterogeneous attachments: half muscle, half tendon (Fig. 49).
Tendons Constructed from dense connective tissue, they have high tensile strength. They are white and shiny. The tendons of flat muscles, such as the obliques, form flat tendon extensions called aponeuroses (aponeurosis). Longus muscles have long, thin cylindrical tendons. Tendons are firmly attached to the bones, fused with the periosteum and even penetrating into the substance of the bone.

Rice. 49. Scheme of the beginning and attachment of the muscle: 1 - muscle bundles; 2 - tendon
A number of signs are used to name muscles. Some muscles are named based on their external shape: deltoid, rhomboid; others - by function: flexors, extensors, abductors, adductors; third - by the number of heads or structure: biceps, semitendinosus; fourth - by location: occipital, gluteal; fifth - at the place of origin and attachment: mylohyoid, sternocleidomastoid; sixth - in the direction: rectus, oblique, transverse abdominal muscles.
Muscle fibers can have different directions relative to the tendon axis. If the fibers are located obliquely and on one side of the tendon, then the muscle is called unipennate (m. unipennatus), if the muscle fibers lie on both sides of the tendon, then the muscle is called bipinnate (m. bipennatus). The muscle fibers can run in a fan-like pattern, creating a powerful tendon (for example, the temporalis muscle). If muscle fibers are concentrated around natural openings, sphincters are formed (t. sphincter); for example, muscles around the mouth, eyes.
Accessory muscle apparatus
The auxiliary apparatus of muscles includes fascia, bursae, synovial sheaths, muscle blocks and sesamoid bones.
Fascia(fasciae) They are dense connective tissue plates. There are subcutaneous superficial fascia and deep intrinsic fascia.
Superficial fascia (fascia superficialis) constructed of loose fibrous connective tissue. It is located under the skin and covers the entire body in a continuous layer with the exception of the head. Bundles of fascia, located in different directions, separate the fatty lobules of subcutaneous fatty tissue from each other. Many areas of the superficial fascia contain greater or lesser amounts of fat. On the soles of the feet and on the palms, fat forms elevations that perform a protective function.
Own fascia (fascia propria) consists of fibrous tissue and is better developed than the superficial one. Enveloping a muscle or group of muscles, its own fascia forms fascial sheaths for them with openings for the passage of blood vessels and nerves. Fascia is not equally developed everywhere. Where the muscles are stronger, the fascia is better expressed

Rice. 50. Osteofascial and fascial sheaths of the muscles of the lower third of the right thigh: 1 - lateral intermuscular septum of the thigh; 2 - fascial sheath of flexors; 3 - sciatic nerve; 4 - femur; 5 - femoral artery and vein; 6 - fascial sheath of the sartorius muscle; 7 - medial intermuscular septum of the thigh; 8 - osteofascial extensor sheath; 9 - fascia lata
(for example, on the lower extremities). If the muscles are located in several layers, then the own fascia splits into plates - superficial and deep. In some places, the fascia itself forms fibrous processes between muscle groups, intermuscular septa (septa intermuscularia), which penetrate deep and fuse with the periosteum.
There are 2 types of muscle sheaths: fascial, formed by fascia, and osteofascial, formed by fascia and bones (Fig. 50). In some muscles, such as the gluteus maximus, the fascia has lamellar processes that penetrate between individual muscle bundles.
Thanks to intermuscular and intramuscular septa, fascia provides support for muscles, blood vessels, nerves, and internal organs. The muscle can originate from the fascia or attach to it. Fascia promotes muscle contraction in a certain direction and prevents it from moving to the sides; it is a soft framework for muscles. When the integrity of the fascia is violated, the muscles in this place protrude, forming a muscle hernia. Fascia is easily separated from the surrounding connective tissue and the muscles they cover, to which they are connected by the perimysium. In certain areas of the human body (for example, gluteal, deltoid), fascia covering the muscles sends

Rice. 51. Synovial tendon sheath:
a - cross section; b - longitudinal section; 1 - fibrous layer; 2 - synovial layer; 3 - tendon; 4 - synovial cavity; 5 - mesentery of tendon (mesotendinium)
connective tissue septa between individual bundles of muscle fibers, thereby increasing the connection between the fascia and the muscles.
Muscle movements are facilitated bursae(bb. synoviales)- closed cavities filled with synovial fluid. Based on their location they are divided into tendon, articular And subcutaneous Tendons are usually located on the limbs between the tendons, articular - in the area of the joints, sometimes connecting to their cavity. Subcutaneous bags are located in areas of the body that experience significant friction or pressure (for example, the knee joint capsule). Synovial vagina(vag. synovialis) similar to a two-layer tube (Fig. 51). The synovial tendon sheaths are closed and filled with synovium. They consist of two layers: outer fibrous and inner synovial. The synovial has 2 layers: the inner one, tightly adjacent to the tendon, is the peritendinium. (peritendineum) and external - epitendinium (epitendineum). The inner leaf is connected to the outer along the length where the friction is weakest, forming the mesentery of the tendon - mesotendinium (mesotendineum), through which blood vessels and nerves pass into the tendon.
Muscle block(trochlea muscularis) is formed in those places where the muscle changes direction and is thrown over bone and fibrous formations. Thanks to the block, the muscle does not move to the side. A synovial bursa is located between the tendon and the block.
Sesamoid bones(ossa sesamoidea) located in the thickness of the tendons near the place of their attachment to the bones. Sesamoid braids
These increase the angle of attachment of the tendon to the bones and thereby help increase muscle strength.
Muscle as an organ
A muscle is an organ consisting of striated (skeletal) muscle fibers held together by loose connective tissue in which blood vessels and nerves pass. Muscle fibers are connected by interfascicular connective tissue - endomysium(endomysium). Individual muscle bundles covered with endomysium are called 1st order bundles. Through layers of connective tissue - perimysium(perimysium), they are combined into bundles of 2nd and 3rd orders. The outside of the muscle is covered by a connective tissue membrane - epimysium(epimysium)(Fig. 52).
If a muscle extends over a joint or from one bone to another, it is called single-joint, and if it goes past two or more joints - biarticular or multi-joint. Muscles not only move the specific parts of the skeleton to which they are attached, but can also facilitate more complex movements by changing the position of bones. Individual muscles or a group of muscles that take part in movements that are opposite in direction are called antagonists. For example, the muscles that flex the foot are antagonistic to the muscles that extend it. Muscles involved in the same movement and located on the same side of the joint are called synergists. Monoarticular muscles of uniaxial joints always perform only one function in relation to these joints. For example, the brachialis muscle is a flexor of the forearm, and the triceps brachii muscle is its antagonist. Many muscles perform more complex functions, being either antagonists or synergists in relation to each other. Thus, the biceps brachii muscle, together with the pronator teres, flexes the forearm, but at the same time it can rotate the radius outward, and the pronator teres rotates it inward. Different parts of the same muscle can perform different functions. For example, if the anterior bundles of the gluteus medius muscle contract, the thigh rotates inward; if posterior, the hip rotates outward; When the entire muscle contracts, the hip abducts.
The muscle, spreading over the joints, connects various bone points to which it is attached with its ends. The proximal end is usually considered the beginning of the muscle or fixed point

Rice. 52. Muscle structure:
1 - muscle as a whole; 2 - epimysium; 3 - perimysium; 4 - bundle of muscle fibers; 5 - individual muscle fibers surrounded by endomysium and blood vessels; 6 - myofibril (contractile structure of muscle fiber); 7 and 8 - molecules of actin and myosin proteins, the interaction of which ensures the contraction of the myofibril
(punctum fixum), opposite, distal end - moving point (punctum mobile). However, with some movements, a fixed point can become mobile and vice versa.
Muscles have a network of blood vessels through which nutrients and oxygen are delivered with the blood, and carbon dioxide and metabolic products are carried out. During muscle work, increased metabolism occurs in them with the release of a significant amount of heat. Arteries depart from the nearest arterial trunks and penetrate the muscle belly from the inner side, the most protected. The places where arteries, veins and nerves enter are called neurovascular gate of the muscle. The location of these gates is important during surgical interventions. Veins are formed from the intramuscular venous network. Each artery is accompanied by two veins, which emerge from the hilum of the muscle and empty into nearby venous vessels.
Muscle contraction occurs under the influence of impulses arising in the central nervous system. Muscles contain motor and sensory nerve endings. From the central nervous system, along motor (efferent) nerve fibers, excitation enters the muscle, to neuromuscular endings of various shapes, and the muscle contracts. Sensitive (afferent) fibers send impulses from the muscle to the central nervous system, signaling the state of the muscle at the moment. Sensory endings in muscles have a neuromuscular spindle, which is an organ of muscle sense. In addition to efferent and afferent ones, sympathetic nerve fibers approach the muscles, which cause a certain contraction in the muscle, called muscle tone.
Muscle work
The main property of muscle tissue is contractility. By contracting, the muscle produces mechanical work. The amount of mechanical work performed by a contracting muscle is expressed in kilograms as the product of the weight of the load lifted by the muscle and the height of the lift. The force exerted by a muscle depends on the number of its muscle fibers, i.e. The thicker the muscle, the stronger it is. The length of the muscle belly determines the height of the load; on average, a muscle shortens by approximately half its length during full contraction. During complex movements, several groups contract
muscles at the same time, and the nature of their contraction and participation in movement are not the same. Distinguish overcoming, yielding And holding muscle work. By overcoming we mean work in which the muscle overcomes resistance. In the case of yielding work, the muscle becomes tense, gradually yielding to the action of gravity. Restraining work is understood as a state of a muscle in which its contraction balances the action of resistance, as a result of which movement does not occur.
The muscles act on the bones, which are connected to each other by joints, so that a lever of one kind or another is obtained. In mechanics, levers are distinguished: first and second kind. In a lever of the first kind, or balance lever, the fulcrum is located between the points of application of forces. The distance from the point of application of force to the point of support is called the lever arm, and the distance from the point of support to the point of resistance is called the resistance arm. The condition for equilibrium of a lever is the equality of the product of the magnitude of the force and the length of the arms. An example of a balance lever would be atlanto-occipital joint(Fig. 53, a).
The second type lever comes in two types. With the first type of lever (force lever) resistance is observed between the fulcrum and the point of application of force. The shoulder force of muscle traction is greater than the shoulder force of gravity. An example of a lever of force is the foot during lifting onto the heads of the metatarsal bones (Fig. 53, b). The place of support in this case is the heads of the metatarsal bones, through which the axis of rotation of the entire foot passes. The force of the muscular pull coming from the heel bone upward in the direction of the pull of the triceps surae muscle has a greater leverage than the force of gravity. The force of gravity is transmitted through the bones of the lower leg to the foot and presses directly on the talus bone, thereby promoting the descent of the foot.
Second type of lever (speed lever) characterized by the fact that the point of application of muscle traction is located near the axis of rotation and the shoulder of muscle traction is smaller than the resistance shoulder. An example of this type of lever is elbow joint when bending. The fulcrum lies in the elbow joint, the point of application of force is in the area of the tuberosities of the ulna and radius, i.e. somewhat anterior to the fulcrum, the point of resistance is at the distal end of the arm, i.e. significantly further from the fulcrum. Such a lever leads to a gain in speed, but a loss in strength (Fig. 53, c).

Rice. 53. Diagram of the action of muscles on bone levers: a - balance lever; b - lever of force; c - speed lever; A - fulcrum; B - point of application of force; B - point of resistance
When contracting, different muscles develop different forces. This strength depends on a number of morphological features. For example, the more muscle fibers, the stronger the muscle. If we compare a muscle with parallel fibers and a pennate muscle, then with the same volume, the pennate muscle will be stronger, since the number of fibers in it is greater.
Equally important for the manifestation of muscle strength is the way they are attached to the bones. The larger the area of muscle support on the skeleton, the better the conditions for the manifestation of its strength. The strength of a muscle depends largely on the angle at which it attaches to the bone. The closer this angle is to the right angle, the greater the component of the force directed toward movement in the joint, and, therefore, the muscle expends more force directly to move the bone link in space. Muscle strength depends on the mass of muscle tissue, the location of the muscles themselves, and their tension. Athletes and physically developed people have greater muscle strength than people who do not engage in physical labor. Physical exercise and hard physical labor help to increase the volume and thicken the muscles. In older people, muscle volume decreases somewhat, as a result of which their strength decreases.
In addition to the described morphological conditions, the degree of its excitation under the influence of the central nervous system is of great importance for the manifestation of muscle strength. The stronger the stimulating impulses coming from the central nervous system, the greater the strength the muscle develops. There is a certain relationship between muscle strength and its cross-section. The larger the diameter of the muscle, the stronger it is. It is believed that 1 cm 2 of muscle cross-section corresponds to a force of about 8-10 kg.
The concept of statics and dynamics of the human body
Muscle work can be divided into myostatic and myodynamic.
Myostatic work expressed in holding parts of the body or the whole body in a certain position. In this position, the force of gravity acting on the body is balanced with the counteracting reaction of the support. To fix a certain position of the body, muscles that maintain balance actively work. With this
When moving a body, the action of external forces does not cause movement. For example, the muscles, through their supporting work, ensure the vertical position of the body, although external forces (gravity) continue to act on it. Therefore, the myostatic body position is a temporarily balanced position, which will be followed by active movements.
Myodynamic work is caused by active muscle variability associated with body movement. Any movement of the body is accompanied by a change in speed (accelerated, slow or uniform movement) and direction (rectilinear, curvilinear, rotational movement). The movement of individual parts of the body in relation to objects surrounding it is called relative movement.
The body or its parts can be affected by internal (muscle traction, inertia) and external (gravity, ground reaction, air resistance, etc.) forces. Interacting with each other, internal and external forces determine the shape and character of the body and its parts: the posture changes with the movement of the center of gravity, the body and its parts can make accelerated, uniform or slow motion.
The movements of the human body performed by skeletal muscles are extremely diverse. Based on mechanical characteristics, they can be divided into translational, rotational and complex. When a body moves forward, its parts move along identical trajectories. During rotational movement, all parts of the body move in circles, the centers of which are located on the same straight line, called the axis of rotation. With complex movement, parts of the body perform simultaneously translational and rotational movements.
Any body moving freely in space has 6 degrees of freedom in the form of translational and rotational movements in 3 dimensions (up and down, forward and backward, right and left). If a body is fixed at one point, then it cannot perform translational motion, but can rotate about 3 axes, i.e. has 3 degrees of freedom. If a body is fixed at two points, then it has 1 degree of freedom and can rotate around one axis. Ball-and-socket joints have three degrees of freedom, ellipsoidal, saddle-shaped and condylar joints have two, and cylindrical and trochlear joints have one.
Center of gravity
Under center of gravity of any body in mechanics is meant the point of application of the resultant of several multidirectional gravity forces acting on its individual parts.
The position of the center of gravity of the human body is of great importance for maintaining balance while standing and during various movements. The human body is heterogeneous, so its center of gravity does not coincide with the center of the body and changes depending on the movement of body parts in space. A person stands steadily if the vertical line descended from the center of gravity is in the center of the area formed by the feet. As soon as you lean forward or to the side and draw a plumb line from the center of gravity beyond the support area, the person begins to fall. To prevent this from happening, place your leg in the direction of the fall, thereby moving the support area.
The density of the upper half of the human body is less than that of the lower half. It has been experimentally established that with a “military” posture, the center of gravity is located at the level of the second sacral vertebra, and the plumb line from the center of gravity runs 3 cm anterior to the ankles.
The position of the center of gravity of the human body is very variable and depends on age, gender, constitution, height, as well as physical development. For example, in men the center of gravity is slightly higher than in women, and in children at an early age it is higher than in adults. The stronger the body is, the wider the support area and the lower the center of gravity.
Questions for self-control
1.What do the muscles of the head, neck and face develop from?
2.What structures belong to the auxiliary apparatus of muscles? What is the main function of each structure?
3.Which muscles are called antagonists and synergists? Give an example.
4.List the levers of muscles acting on bones. Give their characteristics.
5. How are myostatic and myodynamic muscle work characterized?
6.What is meant by the center of gravity of the human body? What significance does it have?
MUSCLES AND FASCIA OF THE TORSO
The muscles and fascia of the trunk are divided according to their location into suboccipital muscles, muscles of the back, chest, abdomen And crotch. The muscles of the trunk are paired and are located symmetrically - on the right and left.
Development of trunk muscles
Skeletal muscles appear in the 4th week of embryonic development from myotomes. Myotome cells - myoblasts - differentiate and turn into striated skeletal muscle fibers. The dorsal part of the myotomes, located next to the spinous processes of the vertebrae, gives rise to the muscles of the back; the muscles of the neck, chest and abdomen are formed from the ventral part of the myotomes.
The innervation of the dorsal and ventral muscles of the trunk is different: the dorsal muscles are innervated by the posterior branches of the spinal nerves, the ventral ones by the anterior ones.
Subsequently, a connective tissue septum grows into the myotomes, dividing them into superficial and deep layers and, accordingly, muscle groups. Simultaneously with the development of the back muscles, the formation of the connective tissue cover - fascia - occurs. Most developed and well expressed thoracolumbar fascia.
The diaphragm is formed from the cervical myotomes. The emerging muscle rudiments of the diaphragm in the neck move down, where, merging, they form a muscle-tendon plate that covers the lower aperture of the chest.
Back muscles
Back(dorsum)- back surface of the body and neck; at the top it turns on neck- the back surface of the neck and reaches the external occipital protrusion, is limited from below by the lateral edges of the sacrum, coccyx and iliac crests, laterally - by the posterior axillary line.
The back muscles are divided into two groups based on their origin and position: superficial, including the muscles of the shoulder girdle, - truncopetal (i.e., in the process of development, moved from the limb to the torso), as well as muscles attached to the ribs, and deep, formed from the dorsal parts of the myotomes, i.e. autochthonous.

Rice. 54.1. Back muscles:
1 - latissimus dorsi muscle; 2 - trapezius muscle; 3 - semispinalis capitis muscle; 4 - splenius capitis muscle; 5 - muscle that lifts the scapula; 6 - superior posterior serratus muscle; 7 - rhomboid major muscle; 8 - muscle that straightens the spine; 9 - serratus posterior inferior muscle
The superficial muscles of the back are separated from the deep ones by a well-defined thoracolumbar fascia (Fig. 54).
Superficial back muscles
1. Trapezius muscle(m. trapezius) has a triangular shape; its base faces the spinous processes of the vertebrae, and the apex

Rice. 54.2. Deep back muscles:
1 - internal oblique abdominal muscle; 2 - lower posterior serratus muscle; 3 - superior posterior serratus muscle; 4 - splenius capitis muscle; 5 - semispinalis capitis muscle; 6 - rectus capitis posterior minor muscle; 7 - rectus capitis posterior major muscle; 8 and 9 - superior and inferior oblique muscles of the head; 10 - longissimus capitis muscles; 11 - spinalis capitis muscle; 12 - longissimus muscle; 13 - iliocostal muscle; 14 - transverse abdominis muscle
on - to the shoulder blade. The muscle starts from the occipital bone, the spinous processes of the VII cervical and all thoracic vertebrae; attaches to the acromion and scapular spine.
Function: the upper muscle bundles raise the scapula, the middle ones bring it closer to the spine, the lower ones lower it. With fixed shoulder blades and bilateral contraction, she throws her head and neck back.
Innervation: accessory nerve, C II -C IV.
2.Latissimus dorsi muscle(m. latissimus dorsi) begins from the spinous processes of the 5-6 lower thoracic vertebrae, from all lumbar vertebrae, the dorsal surface of the sacrum, from the iliac crest; attaches to the crest of the lesser tubercle of the humerus.
Function: rotates the humerus inward, lowers the raised arm, pulls the lowered arm back to the median plane. With fixed hands, it participates in the act of inhalation.
Innervation: thoracodorsal nerve, C VII -CV III.
3.Rhomboid major and minor muscles(mm. rhomboideus major et minor) begin from the spinous processes of the VI-VII cervical and 4 upper thoracic vertebrae; are attached to the medial edge of the scapula.
Function: bring the shoulder blades closer to the spine and lift them up.
4.M levator scapula muscle(m. levator scapulae), starts from the transverse processes of the 4 upper cervical vertebrae; attaches to the upper corner of the scapula.
Function: raises the scapula; when the scapula is fixed, tilts the cervical spine to the side.
Innervation: dorsal nerve of the scapula, C IV -C V.
5.Serratus posterior superior(m. serratus posterior superior) lies under the rhomboid muscle. It starts from the spinous processes of the two lower cervical and two upper thoracic vertebrae and goes down; attaches to ribs II-V.
Function: raises the ribs.
Innervation: intercostal nerves, Th I - Th IV.
6.Serratus posterior inferior muscle(m. serratus posterior inferior) starts from the spinous processes of the two lower thoracic and two upper lumbar vertebrae; attaches to the 4 lower ribs.
Function: lowers the ribs.
Innervation: intercostal nerves, Th IX -Th XII.
Deep back muscles
The deep muscles of the back include 2 isolated muscle tracts - medial and lateral, located in the osteofibrous canal, in the grooves between the spinous and transverse processes of the vertebrae and the angles of the ribs. The medial tract is represented by short muscles lying deep in the osteofibrous canal; the lateral lies superficially and is formed by long muscles. In the back of the neck, on top of these two tracts is located splenius muscle of the neck.
Muscles of the medial tract: transverse spinous(m. transversospinal) And interspinous muscles(mm. interspinales). The transverse spinalis muscle extends from the sacrum to the occipital bone and includes the semispinalis, multifidus, and rotator cuff muscles.
Function: straighten the spine, when contracting on one side, tilt the spine and torso to the side, rotate the spine.
In the back of the neck are located suboccipital muscles(mm. suboccipitales): anterior, lateral, large and small posterior muscles of the head, upper And inferior oblique capitis, splenius capitis And longus capitis muscle.
Function: straighten the head, rotate it together with the atlas around the odontoid process.
Muscles of the lateral tract: erector spinae muscle
(m. erector spinae), consists of the iliocostal, longissimus and spinalis muscles.
Function: straighten the back, lower the ribs and take part in maintaining balance.
The deep muscles of the back are innervated by the posterior branches of the cervical, thoracic and lumbar spinal nerves.
Fascia of the back
There are 3 fasciae in the back area: superficial, nuchal, lumbothoracic.
Superficial fascia is weakly expressed and is part of the general subcutaneous fascia.
Lumbothoracic fascia(fascia thoracolumbalis) consists of two leaves (lamellas) - superficial and deep (Fig. 55). The superficial layer covers the inferior and superior serratus muscles, forms fascial sheaths for the latissimus dorsi muscle,

Rice. 55. The thoracolumbar fascia and its plates. Horizontal section, top view:
1 - deep plate of the thoracolumbar fascia; 2 - psoas major muscle; 3 - transverse process of the lumbar vertebra; 4 - body of the lumbar vertebra; 5 - spinous process; 6 - muscle that straightens the spine; 7 - superficial plate of the thoracolumbar fascia; 8 - junction of the superficial and deep plates of the thoracolumbar fascia; 9 - quadratus lumborum muscle; 10 - external oblique abdominal muscle; 11 - internal oblique abdominal muscle; 12 - transverse abdominal muscle; 13 - left kidney; 14 - intra-abdominal fascia; 15 - peritoneum
rhomboid and trapezius muscles. The deep layer covers the erector spinae muscle. At the top, the superficial layer covers the splenius and semispinalis muscles of the head and neck, where it thickens, receiving the name nuchal fascia(fascia nuchae).
Chest muscles
Breast- part of the body, limited at the top by a conventional line running from the jugular notch of the sternum, further along the collarbone to the acromioclavicular joint, VII cervical vertebra; below it starts from the xiphoid process of the sternum, continues along the costal arch (X rib), then along the XI-XII ribs and ends at the XII thoracic vertebra.
Chest muscles are divided into two groups: muscles of the chest that attach to the upper limb, And own muscles breasts (autochthonous). The diaphragm, which separates the thoracic cavity from the abdominal cavity, is also considered here (Fig. 56, 57).

Rice. 56.Superficial and deep muscles of the chest and abdomen, front view: 1 - pectoralis major muscle (sternocostal part); 2 - pectoralis major muscle (clavicular part); 3 - trapezius muscle; 4 - sternocleidomastoid muscle; 5 - pectoral fascia (deep plate); 6 - pectoralis minor muscle; 7 - deltoid muscle; 8 - serratus anterior muscle; 9 - external oblique m yshty; 10 - rectus abdominis muscle; 11 - transverse abdominal muscle; 12 - internal oblique abdominal muscle; 13 - pyramidalis muscle

Rice. 57. Muscles of the trunk, right view. The scapula is retracted posteriorly, the pectoralis major and minor, the external oblique and the gluteus maximus are removed; The gluteus medius muscle is cut and partially removed: 1 - inferior gemellus muscle; 2 - internal obturator muscle; 3 - superior gemellus muscle; 4 - piriformis muscle; 5 - gluteus minimus; 6 - latissimus dorsi muscle; 7 - serratus anterior muscle; 8 - teres major muscle; 9 - subscapularis muscle; 10 - internal intercostal muscles; 11 - external intercostal muscles; 12 - internal oblique abdominal muscle; 13 - gluteus medius muscle
Muscles of the chest that attach to the upper limb
1.Pectoralis major muscle(m. pectoralis major) consists of 3 parts: clavicular (pars clavicularis), starting from the medial end of the clavicle; sternocostal (pars sternocostalis)- from the sternum and cartilages of the II-VII ribs; abdominal (pars abdominalis)- from the wall of the vagina of the rectus abdominis muscle. The muscle is attached by a common tendon to the crest of the greater tubercle of the humerus. The deltoid-pectoral groove is formed between the edge of the clavicular part and the edge of the deltoid muscle. (sul. deltoideopectoralis), which at the top turns into the triangle of the same name. Passes in the furrow v. cephalica.
Function: lowers the raised arm, pulls it forward, and simultaneously rotates the humerus inward. When the hand is fixed, it raises the ribs, thereby participating in the act of inhalation.
2.Pectoralis minor muscle(m. pectoralis minor) starts from III-V ribs; attaches to the coracoid process of the scapula.
Function: pulls the scapula down and medially, with a fixed scapula, raises the ribs.
Innervation: medial and lateral thoracic nerves, C V -C VIII.
3.Subclavius muscle(m. subclavius) starts from the first rib; attached to extremitas acromialis claviculae.
Function: pulls the collarbone down, with a fixed collarbone raises the 1st rib.
Innervation: subclavian nerve, C V -C VI.
4.Serratus anterior muscle(m. serratus anterior) begins with teeth from the 8-9 upper ribs; attaches to the medial edge of the scapula and to its lower angle.
Function: pulls the lower angle of the scapula forward and laterally, thereby raising the arm above the horizontal line; with a fixed shoulder blade, it raises the ribs, participating in the act of inhalation.
Innervation: long thoracic nerve, C V -CV III.
Own chest muscles
1. External intercostal muscles(mm. intercostales externi) located in the intercostal spaces from the spine to the costal cartilages. They start from the lower edge of the overlying rib, go obliquely down and forward; are attached to the upper edge of the underlying rib.
Function: raise the ribs, participating in the act of inhalation.
Innervation: intercostal nerves, Th 1 -Th XI.
2.Internal intercostal muscles(mm. intercostales interni) lie under the outer ones and have the opposite direction of muscle fibers, located along the length from the sternum to the corners of the ribs.
Function: lower the ribs, participating in the act of exhalation. Innervation: intercostal nerves, Th I -Th XI.
3.Subcostal muscles(mm. subcostales) unstable, located in the posterior part of the chest on the inner surface of the ribs, outward from the corners. They begin and insert as internal intercostal muscles, but extend over one or two ribs.
Function: lowers the ribs.
Innervation: intercostal nerves, Th VIII - Th XI.
4.Transverse thoracis muscle(m. transversus thoracis) starts from the posterior surface of the sternum, attaches to the III-VI ribs.
Function: lowers the ribs.
Innervation: intercostal nerves, Th III - Th VI.
Fascia of the chest
Fascia is distinguished on the chest: superficial, thoracic, clavipectoral, external intercostal And intrathoracic.
1.Superficial fascia weakly expressed, forms a capsule for the mammary gland.
2.Pectoral fascia(fascia pectoralis) has 2 leaves: superficial and deep. They form the sheath of the pectoralis major muscle.
3.Clavipectoral fascia(fascia clavipectoralis) forms the sheath of the subclavian and pectoralis minor muscles. A cellular subpectoral space is formed between the pectoral and clavipectoral fascia. Below, at the lower edge of the pectoralis major muscle, the superficial and deep layers of the pectoral fascia join, passing into the axillary fascia.
4.External intercostal fascia covers the external intercostal muscles.
5.Intrathoracic fascia(fascia endothoracica) lines the inner surface of the chest, passing onto the diaphragm.
Diaphragm
Diaphragm(diaphragm)- an unpaired thin tendon-muscular plate of a dome shape. The diaphragm closes the lower opening of the chest, separating the chest cavity from the abdominal cavity (Fig. 58). The diaphragm begins with muscle-tendon fibers from the bone formations that limit the lower opening of the thoracic

Rice. 58.Diaphragm, bottom view, from the abdominal cavity: 1 - quadratus lumborum muscle; 2 - psoas minor muscle; 3 - psoas major muscle; 4 - fascia iliaca; 5 - transverse fascia; 6 - psoas major muscle (partially removed); 7 - iliacus muscle; 8 - intertransverse muscles; 9 - lateral arcuate ligament; 10 - medial arcuate ligament; 11 - lumbar part of the diaphragm; 12 - esophageal opening; 13 - opening of the inferior vena cava; 14 - tendon center
cells. The muscle fibers, moving upward, pass into the tendon stretch, which occupies a central position and is called the tendon center (centrum tendineum). In its right side there is an opening of the inferior vena cava (for. vv. cavae).
Depending on the location of the origin of the muscle fibers of the diaphragm, 3 parts are distinguished in it: lumbar, costal, sternal.
Lumbar part(pars lumbalis) the most powerful, consists of two legs - right and left (crus dextrum et sinistrum). At the level of the XII thoracic and I lumbar vertebrae, the right and left legs converge, limiting the aortic opening (hiatus aorticus), through which the aorta and the thoracic lymphatic duct lying behind it pass. Then the legs partially cross again and, diverging again, form the esophageal opening (hiatus esophageus) for the passage of the esophagus and vagus nerves. Between the muscle bundles of the legs themselves, the great splanchnic nerve and azygos vein pass on the right, and the same nerve and semi-gypsy vein on the left.
Rib part(pars costalis) begins with teeth from the inner surface of the lower 6 ribs. The muscle fibers run vertically upward and inward, curl in an arc and end in the tendon center.
Sternal part(pars externalis) represents the smallest part of the diaphragm. It starts from the xiphoid process in two bundles that rise upward and end in the tendon center.
The diaphragm on the side of the thoracic cavity is covered with intrathoracic fascia, on the side of the abdominal cavity - with intra-abdominal fascia. Serous membranes are adjacent to the fascia: on the side of the chest cavity - the diaphragmatic pleura, in the middle part of the diaphragm - the pericardium, on the side of the abdominal cavity - the parietal layer of the peritoneum.
Function: diaphragm - respiratory muscle. When it contracts, the dome flattens, lowering by 1-3 cm, and the volume of the thoracic cavity increases. When relaxed, the diaphragm rises upward, and the capacity of the chest decreases.
Innervation: phrenic nerve and intercostal nerves, C III -C V.
Abdominal muscles
Stomach- part of the body located between the chest and pelvis. From above it is limited by the xiphoid process, costal arches and the line connecting the ends of the XII ribs with the spinous processes of the XII thoracic vertebrae; below - the symphysis, the upper branches of the pubic bones, the iliac crests; behind - a line connecting the spinous processes of the lumbar vertebrae. Also considered abdominal cavity and its walls (see “The abdominal cavity and peritoneum”).
There are two groups of abdominal muscles: anterolateral, uniting the rectus, pyramidal and broad muscles (external, internal
early oblique and transverse), and back, represented by the quadratus lumborum muscles (Fig. 59, 60). In the midline, the tendon stretches (aponeuroses) of the vastus lateralis muscles form a fibrous band called white line(linea alba), which runs from the xiphoid process to the symphysis.

Rice. 59.Superficial abdominal muscles:
1 - aponeurosis of the external oblique abdominal muscle; 2 - muscular part of the external oblique abdominal muscle; 3 - latissimus dorsi muscle; 4 - serratus anterior muscle; 5 - subcutaneous adipose tissue and superficial vessels; 6 - spermatic cord entering the inguinal canal

Rice. 60.Inguinal canal, front view. On the right side, the external and internal oblique muscles of the abdomen are cut and turned to the side. On the left side, the anterior wall of the rectus abdominis sheath was removed: 1 - inguinal canal (opened); 2 - spermatic cord; 3 - rectus abdominis muscle; 3a - pyramidal muscle; 4 - deep ring of the inguinal canal; 5 - superficial ring of the inguinal canal; 6 - aponeurosis of the external oblique abdominal muscle; 7 - transverse fascia of the abdomen; 8 - internal oblique abdominal muscle; 9 - transverse abdominal muscle
Approximately in the middle of the white line there is umbilical ring
(anulus umbilicalis), covered by fibrous scar tissue and skin. Sometimes the umbilical ring serves as a site for the formation of umbilical hernias.
Anterolateral abdominal muscle group
1. Rectus abdominis muscle(m. rectus abdominis) steam room, lies on the side of the white line of the abdomen in the tendon sheath. Starts from the V-VII ribs
and the xiphoid process, goes down; attaches to the pubis and symphysis. Along its length it is crossed by tendon bridges (intersectiones tendineae), which in the amount of 3-4 go transversely.
Rectus sheath formed by the aponeuroses of the oblique and transverse muscles and has two plates - anterior and posterior.
Upper 3/4 anterior plate the vagina is formed by the aponeurosis of the external oblique muscle of the abdomen and the anterior layer of the aponeurosis of the internal oblique muscle, back- the posterior layer of the aponeurosis of the internal oblique muscle and the aponeurosis of the transverse abdominal muscle. The anterior plate of the lower quarter of the vagina is formed in front by the aponeuroses of all 3 broad abdominal muscles, and the posterior plate is formed only by the transverse fascia.
2.Pyramidalis muscle(m. pyramidalis) steam room, starts from the pubic bone; attaches to the linea alba.
Function: the pyramidalis muscle and the rectus abdominis muscle stretch the linea alba.
3.External oblique muscle(m. obliquus externus abdominis) steam, the widest of all abdominal muscles. It starts on the lateral surface of the chest from the 8th lower ribs. The muscle bundles go from top to bottom, from outside to inside. At the outer edge of the rectus abdominis muscle, the muscle fibers pass into tendon stretch, forming the anterior plate of the aponeurosis of the rectus abdominis muscle. Attaches to the outer lip of the iliac crest.
The lower edge of the aponeurosis of the external oblique muscle of the abdomen is thrown between the anterior superior iliac spine and the pubic tubercle and is called the inguinal ligament (lig. inguinale), stretched in the form of a trench. The fibers of the inguinal ligament, going down and medially, diverge, forming two legs - medial and lateral, limiting the triangular slit. Medial pedicle (crus mediale) attaches to the symphysis, lateral (crus laterale)- to the pubic tubercle. The medial and lateral crura limit superficial inguinal ring. In the posteroinferior section, between the external oblique muscle of the abdomen in front and the latissimus dorsi muscle in the back, a lumbar triangle (trigonum lumbale); from below it is limited by the iliac crest, the bottom is made up of the internal oblique abdominal muscle. Lumbar hernias can emerge through this triangle.
4.Internal oblique muscle(m. obliquus internus abdominis) steam room, lies under the external oblique muscle of the abdomen. Starts from
thoracolumbar fascia and lateral sections of 2/3 of the inguinal ligament. The muscle bundles run fan-shaped and are attached to the lower edges of the X, XI, XII ribs, forming an aponeurosis, which participates in the formation of the sheath of the rectus abdominis muscle and the linea alba.
5. Transverse abdominis muscle(m. transversus abdominis) steam room, located deeper than the internal oblique muscle of the abdomen. Starting from the inner surface of the six lower ribs, the thoracolumbar fascia and the inner third of the inguinal ligament, it forms an aponeurosis that forms the posterior plate of the rectus sheath and the linea alba.
Fibers are split off from the lower edge of the internal oblique and transverse abdominal muscles in the inguinal canal levator testis muscle(T. cremaster), which, as part of the spermatic cord, exits through the superficial inguinal ring and reaches the testicle.
Function: the muscles of the anterolateral group exert pressure on the insides, forming the so-called abdominal press (prelum abdominale). This pressure promotes emptying of internal organs, for example during bowel movements, urination, childbirth, and vomiting. In addition, the muscles flex the spine, bringing the rib cage closer to the pelvis. The simultaneous contraction of the oblique abdominal muscles causes the torso to rotate to the sides, while the internal and opposite external oblique muscles turn in their direction. By lowering the ribs, the muscles facilitate the act of breathing.
Innervation: intercostal, iliohypogastric and ilioinguinal nerves, Th V - Th XII, L I - L II.
Posterior abdominal muscles
Quadratus lumborum muscle(m. quadratus lumborum) steam room, starts from the iliac crest, from the transverse processes of the 3-4 lower lumbar vertebrae; attaches to the lower edge of the XII rib, the transverse processes of the II-V lumbar vertebrae and to the body of the XII vertebra.
Function: lowers the XII rib, with bilateral contraction it bends the lumbar spine, with unilateral contraction it bends the spine to the side.
Innervation: lumbar plexus, Th XII, L I -L II.
Inguinal canal
Inguinal canal(canalis inguinalis)- the gap through which men pass spermatic cord, and for women - round ligament of the uterus.
It is located in the lower part of the abdominal wall from top to bottom, from outside to inside, from back to front. Its length is 4.0-4.5 cm. The canal has 4 walls and 2 holes. Front the wall is formed by the aponeurosis of the external oblique muscle of the abdomen, back- transverse fascia, top- the lower edges of the internal oblique and transverse abdominal muscles, the lower - the groove of the inguinal ligament. External opening of the channel - superficial inguinal ring(anulus inguinalis superficial)- formed by the legs of the aponeurosis of the external oblique abdominal muscle. Inner hole - deep inguinal ring(anulus inguinalis profundus)- located on the posterior surface of the anterior wall of the abdomen in the form of a depression in the transverse fascia of the abdomen. It corresponds to the lateral inguinal fossa, located outward from the lateral umbilical fold, through which the inferior hypogastric artery passes (see Fig. 60; Fig. 61).

Rice. 61. The relief of the inner surface of the anterior abdominal wall in its lower sections; rear view, from the abdominal cavity:
1 - lateral inguinal fossa; 2 - lateral umbilical fossa; 3 - medial inguinal fossa; 4 - medial umbilical fold; 5 - median umbilical fold; 6 - supravesical fossa; 7 - inferior epigastric artery and veins; 8 - lateral umbilical fold; 9 - bladder; 10 - parietal peritoneum; 11 - vas deferens; 12 - deep inguinal ring
Abdominal fascia
Each abdominal muscle is covered with its own fascia. In the area of the superficial inguinal ring, the fascia continues to the muscle that lifts the testicle and is called fascia cremasterica. On the inside, the transverse muscle is covered with transversalis fascia, which forms part intra-abdominal fascia(fascia endoabdominalis).
In practical terms, the space located between the transverse fascia of the abdomen and the parietal layer of the peritoneum, the so-called preperitoneal space, is very important. (spatium praeperitonialis), which passes posteriorly into the retroperitoneal space (spatium retroperitoniale).
Questions for self-control
1.What groups of back muscles do you know by origin and position? Name these muscles.
2.List the deep muscles of the medial tract of the back. What function do they perform?
3.List the deep muscles of the lateral tract of the back. What function do they perform?
4.What fascia of the back do you know? What do they cover?
5.Name the muscles of the chest that attach to the upper limb. Where do they begin and end, what are their functions?
6.Where do your own chest muscles begin and end? What is their function?
7.What fascia of the chest do you know? What does each fascia form (cover)?
8.Where does each part of the diaphragm begin and end?
9.What groups of abdominal muscles do you know? Name these muscles. 10. How are the walls of the inguinal canal formed?
MUSCLES AND FASCIA OF THE LIMB
Development of muscles and fascia of the limbs
The buds of the limbs appear at the end of the 4th - beginning of the 5th week of the intrauterine period on the lateral surfaces of the body. During the 6-7th week, the limbs grow in length. The muscles of the upper limb develop from the buds of the mesoderm, formed from the anterior parts
catch 4 cervical and 1 thoracic myotomes, muscles of the lower extremities - from the same sections 4 lumbar and 3 sacral myotomes. The mesoderm, from which the muscles of the limbs are formed, is first located dorsal and ventral to the bones of the limbs. The dorsally located mesoderm turns into extensor muscles, abductor muscles and their fascia, and the ventrally located mesoderm turns into flexor muscles, adductor muscles and their fascia. On the lower limb, the extensors move to the anterior surface, and the flexors move to the posterior surface.
Muscles and fascia of the upper limb
Muscles of the upper limb girdle
The connecting link between the free upper limb and the torso is upper, or brachial, a belt whose mobility is ensured by the sternoclavicular joint.
The muscles of the upper limb girdle, or shoulder girdle, covering the shoulder joint on all sides, strengthen it, and when contracted, provide various movements of the upper limb (Fig. 62, 63).
1. Deltoid(m. deltoideus) has a triangular shape, surrounds the shoulder joint from the outside, front and back. Starts from the acromial end of the clavicle, acromion and scapular spine; attaches to the deltoid tuberosity of the humerus.
Function: the anterior muscle bundles flex the shoulder, the posterior ones - straighten, the outer ones - abduct the shoulder to a horizontal position.
Innervation: axillary nerve, C IV -C VII, Th I.
Rice. 62. Muscles of the upper limb girdle:
a - front view: 1 - acromial process; 2 - coracoid process; 3 - subscapularis muscle; 4 - tendon of the long head of the biceps brachii muscle; b - rear view: 1 - supraspinatus muscle; 2 - spine of the scapula; 3 - acromial process; 4 - infraspinatus muscle; 5 - teres minor muscle;
c - shoulder muscles (superficial layer): 1 - subscapularis muscle; 2 - coracobrachialis muscle; 3 - short head of the biceps brachii muscle; 4 - teres major muscle; 5 - latissimus dorsi muscle; 6 - belly of the biceps brachii muscle; 7 - pronator teres; 8 - brachioradialis muscle; 9 - deltoid muscle; 10 - pectoralis major muscle; 11 - long head of the biceps brachii muscle; 12 - synovial sheath of the long head in the cavity of the shoulder joint; d - muscles of the shoulder (deep layer): 1 - coracobrachialis muscle; 2 - brachialis muscle


Rice. 63. Shoulder muscles, rear view:
a: 1 - teres major muscle; 2 - teres minor muscle; 3 - infraspinatus muscle; 4 - supraspinatus muscle; 5 - scapular spine; 6 - deltoid muscle; 7 - long head of the triceps brachii muscle; 8 - lateral head of the triceps brachii muscle; 9 - olecranon; 10 - elbow muscle;
b:1 - three-sided hole; 2 - four-sided hole; 3 - medial head of the triceps brachii muscle
2.Supraspinatus muscle(m. supraspinatus) located in the same fossa of the scapula. Starts from the supraspinatus fossa and fascia, passes under the conical ligament; attaches to the greater tubercle of the humerus and the capsule of the shoulder joint.
Function: abducts the shoulder and tightens the joint capsule, protects it from pinching.
3.Infraspinatus muscle(m. infraspinatus) fills the infraspinatus fossa of the scapula. The muscle fibers, moving outward and upward, pass into the tendon, which is attached to the large tubercle of the humerus.
Function: Rotates the shoulder outward and also retracts the capsule of the shoulder joint.
Innervation: suprascapular nerve, C V -C VI.
4.Teres minor muscle(m. teres minor) lies in the lateral part of the infraspinatus fossa of the scapula. Starts from the infraspinatus fascia and the lateral edge of the scapula; attaches to the greater tubercle of the humerus.
Function: rotates the shoulder outward. Innervation: axillary nerve, C V -C VI, Th I.
5.Teres major muscle(m. teres major) starts from the dorsal surface of the lower angle of the scapula; attaches to the crest of the lesser tubercle of the humerus.
Function: pulls the shoulder back, rotates it inward and leads to the body. Innervation: subscapular nerve, C V -C VI.
6.Subscapularis muscle(m. subscapularis) fills the subscapular fossa. Starts from the costal surface of the scapula and subscapular fascia; attaches to the lesser tubercle of the humerus and articular capsule.
Function: rotates the shoulder inward, pronates, brings the shoulder toward the body and retracts the capsule.
Innervation: subscapular nerve, C V -C VI.
Muscles of the free upper limb
Shoulder muscles
The muscles of the shoulder include long muscles, which are located on the anterior and posterior surfaces of the humerus and form two groups - anterior and posterior, separated by intermuscular medial and lateral septa (septa intermuscularia brachii mediale et laterale).
Anterior group - flexor muscles
1.Biceps brachii(m. biceps brachii) biarticular, acts on the shoulder and elbow joints; has two heads - short and long. The short head starts from the coracoid process of the scapula, the long head starts from the supraglenoid tubercle of the scapula. The tendon of the long head passes into the cavity of the shoulder joint in the intertubercular groove of the humerus, surrounded by the intertubercular synovial sheath (vag. tendenis intertubercularis). In the middle third of the shoulder, both heads join to form a muscle belly, which is attached to the radial tuberosity.
Function: flexes the radial and elbow joints, supinates the forearm.
2.Brachialis muscle(m. brachialis) begins on the anterior surface of the humerus and intermuscular septa; attaches to the ulnar tuberosity.
Function: flexes the forearm.
Innervation: musculocutaneous nerve, C V -C VII.
3.Coracobrachialis muscle(m. coracobrachialis) starts from the coracoid process of the scapula; attaches to the medial surface of the humerus.
Function: flexes the shoulder and pulls it towards the median plane. Innervation: musculocutaneous nerve, C V -C VII.
1.Triceps brachii(m. triceps brachii) located on the posterior surface of the humerus. It starts with three heads. Long head (caput longum) starts from the subarticular tubercle of the scapula; lateral (caput laterale)- from the posterior surface of the humerus; medial (caput mediale)- also from the posterior surface of the humerus. All the heads in the distal part are connected and attached to the olecranon process of the ulna.
2. Elbow muscle(m. anconeus) triangular in shape, starting from the lateral epicondyle of the humerus; attaches to the posterior surface of the proximal end of the ulna.
Function: extends the forearm at the elbow joint. Innervation: radial nerve, C V -C VIII.
Forearm muscles
The forearm muscles are examined in a position of complete supination. According to their function, they are divided into two groups: the anterior group - flexors and pronators, and the posterior group - extensors and supinators (Fig. 64, 65).
Anterior group - flexors of the forearm and hand
1.Brachioradialis muscle(m. brachioradialis) starts from the lateral edge of the humerus and attaches to the lateral surface of the radius above the styloid process.
Function: flexes the forearm and sets the radius in a mid-position between pronation and supination. Innervation: radial nerve, C V -C VI.
2.Pronator teres(m. pronator teres) starts from the medial epicondyle of the humerus, goes down and laterally; attaches to the posterior edge of the radius above its middle.
Function: pronates the forearm and participates in its flexion. Innervation: median nerve, C VI -C VII.
3.Flexor carpi radialis(m. flexor carpi radialis) starts from the medial epicondyle of the humerus; attaches to the base of the second metacarpal bone.
Function: performs palmar flexion of the hand. Innervation: median nerve, C VI -C VII.
4.Palmaris longus muscle(m. palmaris longus) starts from the medial epicondyle, forms a long tendon that passes into the palmar aponeurosis.
Function: flexes the hand, strains the palmar aponeurosis. Innervation: median nerve, C VII -C VIII.
5.Flexor carpi ulnaris(m. flexor carpi ulnaris) located medially. It starts from the medial epicondyle of the humerus and attaches to the pisiform bone.
Function: bends and adducts the hand. Innervation: ulnar nerve, C VII -C VIII.
The listed 5 muscles make up the superficial layer of the forearm flexors. Deeper lie 4 muscles, forming a deep layer.
1. Flexor digitorum superficialis(m. flexor digitorum superficialis) starts from the medial epicondyle of the humerus, the coronoid process of the ulna. At the distal end, the muscle forms 4 tendons that pass through the carpal tunnel to the hand. The tendons are attached to the lateral surface of the middle phalanges of the II-V fingers.
Rice. 64.1. Muscles of the anterior side of the forearm. Surface layer, front view:
I - pronator teres; 2 - flexor carpi radialis; 3 - palmaris longus muscle; 4 - superficial flexor of the fingers; 5 - flexor carpi ulnaris; 6 - flexor retinaculum; 7 - short palmaris muscle; 8 - elevation of the little finger; 9 - palmar aponeurosis; 10 - eminence of the thumb;
II - tendon of the abductor pollicis longus muscle; 12 - flexor pollicis longus;
13 - superficial flexor of the fingers;
14-radialis flexor carpi; 15 - brachioradialis muscle; 16 - aponeurosis of the biceps brachii muscle; 17 - brachialis muscle; 18 - biceps brachii; 19 - medial epicondyle
Rice. 64.2. Flexor digitorum superficialis, anterior view. The pronator teres, flexor carpi radialis, and palmaris longus muscles were removed:
1 - medial epicondyle of the humerus; 2 - humeroulnar head of the superficial flexor digitorum;
3- superficial flexor of the fingers;
4- quadratic pronator; 5 - fascia of the forearm; 6 - palmaris longus tendon; 7 - flexor carpi radialis tendon; 8 - flexor pollicis longus; 9 - radial head of the superficial flexor digitorum; 10 - instep support;
11 - brachioradialis muscle; 12 - brachialis muscle
Rice. 64.3. Flexor digitorum profundus, anterior view. Superficial forearm muscles removed: 1 - medial epicondyle of the humerus; 2 - deep flexor of the fingers; 3 - flexor carpi ulnaris; 4 - pisiform bone; 5 - muscle opposing the little finger; 6 - tendons of the deep flexor of the digitorum; 7 - tendons of the superficial flexor of the fingers (cut off); 8 - adductor pollicis muscle; 9 - flexor pollicis longus tendon; 10 - short flexor pollicis; 11 - muscle opposing the thumb; 12 - pronator quadratus; 13 - flexor pollicis longus; 14 - pronator teres; 15 - long extensor carpi radialis; 16 - brachioradialis muscle; 17 - instep support; 18 - brachialis muscle
Rice. 64.4. Pronator quadratus and pronator teres, anterior view. Other muscles of the anterior side of the forearm were removed: 1 - medial epicondyle; 2 - pronator teres; 3 - ulna; 4 - pronator quadratus; 5 - interosseous membrane of the forearm; 6 - radius; 7 - instep support; 8 - tendon of the biceps brachii; 9 - joint capsule
Rice. 65. Muscles of the back of the forearm, rear view:
1 - lateral epicondyle; 2 - extensor carpi radialis longus; 3 - short extensor carpi radialis; 4 - extensor fingers; 5 - abductor pollicis longus muscle; 6 - short extensor pollicis; 7 - extensor retinaculum; 8 - tendon of the muscle - long extensor of the thumb; 9 - extensor tendon of the index finger; 10 - extensor tendon; 11 - intertendon connections; 12 - extensor tendon of the little finger; 13 - extensor carpi ulnaris; 14 - extensor of the little finger; 15 - extensor carpi ulnaris; 16 - elbow muscle; 17 - olecranon; 18 - triceps brachii muscle
Function: bends the middle phalanges of the II-V fingers and the hand. Innervation: median nerve, C VII -C VIII.
2.Flexor pollicis longus brushes (m. flexorpollicis longus) begins on the anterior surface of the radius; attaches to the base of the distal phalanx of the thumb.
Function: flexes the distal phalanx of the thumb. Innervation: median nerve, C VI -C VIII.
3.Flexor digitorum profundus(m. flexor digitorum profundus) starts from the anterior surface of the ulna. At the distal end of the forearm it forms 4 tendons, which pass in the carpal canal along with the tendons of the superficial flexor of the fingers and are attached to the bases of the distal phalanges of the II-V fingers.
Function: flexes the distal phalanges of the fingers. Innervation: median and ulnar nerves, C VII -Th I.
4.Pronator quadratus(m. pronator quadratus) located in the distal forearm, lies under the deep flexor of the digitorum. Starts from the anterior surface of the ulna; attaches to the anterior surface of the radius.
Function: rotates the radius inward. Innervation: median nerve, C VII -Th I.
Posterior group - extensors of the forearm and hand are located in 2 layers - superficial and deep. Surface layer
1.Extensor carpi radialis longus(m. extensor carpi radialis longus) starts from the lateral edge and from the lateral epicondyle of the humerus; attaches to the base of the second metacarpal bone.
Function: extends and abducts (together with t. flexor carpi radialis) brush. Innervation: radial nerve, C VI -C VII.
2.Extensor carpi radialis brevis(m. extensor carpi radialis brevis) starts from the lateral epicondyle of the humerus; attaches to the base of the third metacarpal bone.
Function: extends the hand. Innervation: radial nerve, C VI -C VIII.
3.Extensor digitorum(m. extensor digitorum) starts from the lateral epicondyle of the humerus, in the distal part it is divided into 4 tendons that pass under the extensor retinaculum (retinaculum extensorum), go to the dorsum of the II-V fingers and attach to the distal and middle phalanges.
Function: extends the second fingers. Innervation: radial nerve, C VI -C VIII.
4.Extensor digitorum(m. extensor digiti minimi) separated from the extensor digitorum, attached to the base of the distal phalanx of the finger.
Function: extends the finger. Innervation: radial nerve, C VI -C VIII.
5.Extensor carpi ulnaris(m. extensor carpi ulnaris) starts from the lateral epicondyle of the humerus, attaches to the base of the metacarpal bone.
Function: extends and adduces (together with m. flexor carpi ulnaris) brush. Innervation: radial nerve, C VII -C VIII. Deep layer
1.Arch support(m. supinator) starts from the lateral epicondyle of the humerus. Attached to the radius.
Function: rotates the radius outward. Innervation: radial nerve, C V -C VI.
2.Abductor pollicis longus muscle(m. abductor pollicis longus), starts from the distal bones of the forearm; attaches to the base of the first metacarpal bone.
Function: abducts the thumb. Innervation: radial nerve, C VI -C VII.
3.Extensor pollicis brevis(m. extensor pollicis brevis) starts from the posterior surface of the radius; attaches to the proximal phalanx of the thumb.
4.Extensor pollicis longus(m. extensor pollicis longus) starts from the back surface of the ulna; attaches to the posterior surface of the distal phalanx of the thumb.
Function: extends the thumb. Innervation: radial nerve, C VI -C VII.
5.Extensor index finger(m. extensor indicis) starts from the back surface of the ulna, near the head; attaches to the extensor tendon of the digitorum, which goes to the index finger.
Function: extends the second finger. Innervation: radial nerve, C VII -C VIII.
Muscles of the hand
There are short muscles on the hand, which form 3 groups on the palmar surface: lateral, medial and middle.
Lateral group. It consists of 4 muscles: abductor pollicis brevis muscle(m. abductor pollicis brevis);flexor pollicis brevis(m. flexor pollicis brevis);muscle that opposes the thumb(m. opponens pollicis);adductor pollicis muscle(m. adductor pollicis). All muscles originate from the carpal bones and the flexor retinaculum; attached to the base of the proximal first phalanx.
Innervation: short flexor and adductor muscle - ulnar nerve, C VII -Th I; short abducens and opposites - by the median nerve, C VI -C VII.
Medial group. The muscles of this group are less developed than the lateral ones. It consists of 4 muscles: abductor digiti minimi muscle(m. abductor digiti minimi);flexor digiti brevis(m. flexor digiti minimi brevis);Opposite little finger muscle(m. opponens digiti minimi). They start from the flexor retinaculum and carpal bones; attached to the proximal phalanx of the little finger and fifth metacarpal bone.
Function: corresponds to the names of the muscles.
Innervation: ulnar nerve, C VII -Th I.
Middle group. This group belongs to lumbrical muscles(mm. lumbricales),palmar and dorsal interosseous muscles(mm. interossei palmares et dorsales).
Function: vermiforms bend the proximal phalanges of the II-V fingers; palmar interosseous brings the fingers together; the back fingers spread.
Innervation: median, ulnar nerves, C VIII -Th I.
Fascia of the upper limb
The superficial fascia of the upper limb is poorly expressed. Own fascia(fascia propria) forms well-defined vaginas for groups and individual muscles. Deltoid fascia(fascia deltoidea) covers the deltoid muscle. Underneath it there is a subdeltoid space that communicates with the tissue of the armpit (fossa).
The fascia lining the armpit is called axillary fascia(fascia axillaris). She goes into her own shoulder fascia(fascia brachii). This fascia, giving off strong medial and lateral

Rice. 66.Synovial sheaths of the hand:
1 - flexor carpi radialis tendon sheath; 2 - common synovial sheath of the digital flexors; 3 - tendon sheath of the flexor pollicis longus; 4 - synovial and fibrous sheaths of the tendons of the fingers
intermuscular septa of the shoulder (septa intermuscularia brachii mediate et laterale), forms 2 osteofascial sheaths: anterior for the flexor muscles of the shoulder and forearm, posterior for the extensor muscles.
Fascia of the forearm(fascia antebrachii) well expressed, covers all muscles of the forearm; forms 3 osteofascial sheaths: anterior, posterior and external. In the anterior are the flexors of the fingers and hand, in the back are the extensors of the fingers and hand, in the outer are the brachioradialis muscle, the long and short radial extensors of the wrist.
In the distal forearm, at the border with the hand, the fascia of the forearm thickens, forming retinaculum of flexor and extensor muscles(retinaculum musculorum flexorum et extensorum), then moves onto the brush, forming palmar aponeurosis(aponeurosis palmaris). On the hand, in addition to the palmar aponeurosis, there are dorsal fascia of the hand(fascia dorsalis manus).
On the palmar surface in the carpal tunnel (canalis carpi), through which the retinaculum of the flexor muscles is thrown, there are 2 synovial sheaths (Fig. 66): for the flexor pollicis longus and common for the tendons of the superficial and

Rice. 67. Synovial sheaths of the tendons of the extensor muscles of the fingers of the right hand, rear view: 1 - extensor retinaculum; 2 - sheath of the tendons of the radial extensor carpi; 3 - tendon sheaths of the abductor pollicis longus muscle and the extensor pollicis brevis muscle; 4 - intertendon connections; 5 - sheath of the extensor tendon of the little finger; 6 - sheath of the extensor tendons of the fingers and the extensor of the index finger; 7 - extensor carpi ulnaris tendon sheath
deep flexor of the fingers, which from the medial side continues without interruption onto the flexor tendon of the little finger up to the distal phalanx. The flexor tendons of the three middle fingers (II, III and IV) have their own separate synovial sheaths. They do not connect to the synovial sheaths of the palm and lie in the osteofibrous canals of the fingers, surrounded by circular and cross ligaments.
On the back of the hand there are 6 synovial sheaths (Fig. 67): in first the tendons of the abductor pollicis longus muscle and the extensor pollicis brevis muscle pass through; in second- tendons of the long and short radial extensors of the hand; V third- tendons of the extensor pollicis longus; V fourth- 4 digital extensor tendons; V fifth- tendon of the extensor muscle of the fifth finger; V sixth- extensor carpi ulnaris tendon.
There are 3 osteo-fibrous spaces in the palm: medial- for the muscles of the little finger, lateral- for the muscles of the thumb
And average- for the tendons of the superficial and deep flexor of the fingers and lumbrical muscles.
Elements of topography of the upper limb
Throughout the upper limb there are various kinds of gaps between the muscles, which are of practical interest, since blood vessels and nerves pass through them.
Axillary fossa(fossa axillaris) bounded anteriorly by the lower edge of the pectoralis major muscle, behind- the lower edge of the latissimus and teres major muscles, medially- a conventional line connecting the edges of these muscles on the chest, laterally- a conditional line connecting the same edges on the inner surface of the shoulder. Upon removal of the axillary fascia, it is revealed axillary cavity(cavum axillare), her front wall formed by the pectoralis major and minor muscles, back- latissimus dorsi, teres major and subscapularis muscles, medial- serratus anterior muscle, lateral- humerus, coracobrachialis muscle and short head of the biceps muscle. The axillary cavity is filled with fatty tissue, lymph nodes, vessels and nerves, narrows upward and communicates with the neck through the upper aperture.
There are 2 openings on the posterior wall of the axillary fossa: medial trilateral (for. trilaterum), limited by the teres major and subscapularis muscles and the long head of the triceps muscle, as well as the lateral quadrilateral (for. quadrilaterum), limited by the same muscles and humerus. Vessels and nerves pass through these openings. In the axillary cavity there are 3 triangles: clavipectoral (trigonum clavipectorale), bounded above by the clavicle and below by the upper edge of the pectoralis minor muscle; chest (trigonum pectorale), corresponding to the contours of the pectoralis minor muscle; submammary (trigonum subpectorale), the base is facing laterally and located between the lower edges of the pectoralis minor (above) and major (bottom) muscles. The shoulder contains the medial groove (sul. bicipitalis medialis), containing the neurovascular bundle, and the lateral groove (sul. bicipitalis lateralis). They are located on the sides of the biceps brachii muscle.
On the back of the shoulder, between the medial and lateral heads of the triceps muscle and the humerus, is located brachial canal(canalis humeromuscularis).
On the anterior surface of the elbow joint is cubital fossa(fossa cubiti), bounded laterally by the brachioradialis muscle, medially by the pronator teres muscle. The bottom of the fossa is formed by the brachialis muscle.
There are 3 grooves on the front surface of the forearm.
Radial sulcus(sul. radialis) located between the brachialis muscle and the flexor carpi radialis. Ulnar groove(sul. ulnaris) limited by flexor carpi ulnaris and flexor digitorum superficialis. Median sulcus(sul. medianus) located between the flexor carpi radialis and the flexor digitorum superficialis.
Questions for self-control
1.List the muscles of the shoulder girdle. Indicate their origin, attachment and function.
2.List the shoulder muscles by group. Indicate their origin, attachment and function.
3.What muscles belong to the anterior muscle group of the forearm? Where do they begin and attach, what is their function?
4.What muscles belong to the posterior group of muscles of the forearm? Where do they begin and attach, what is their function?
5.Name the muscles of the hand by group. Where do they begin and attach?
6.What fascia of the upper limb do you know? What do they form (lining)?
7.What is the axillary fossa limited by?
8.What are the walls of the axillary cavity formed by?
9.What muscles are the ulnar fossa limited by?
Muscles and fascia of the lower limb
Muscles of the lower limb girdle
The muscles of the lower limb girdle (Fig. 68-70) - the pelvis - surround the hip joint. They start from the sacrum, pelvic bones and spine, and are attached to the proximal end of the femur. Topographically, they are divided into two groups: internal and external pelvic muscles.
Internal pelvic muscles
1. Iliopsoas muscle(m. iliopsoas) consists of two muscles: ileal(m. iliacus), starting in the iliac fossa,

Ab
Rice. 68.Thigh muscles, front view:
a - superficial layer: 1 - iliacus muscle; 2 - psoas major muscle; 3 - pectineus muscle; 4 - long adductor muscle; 5 - thin muscle; 6 - sartorius muscle; 7 - rectus femoris muscle; 8 and 9 - vastus medialis and lateral muscles; 10 - tensor fascia lata; b - part of the muscles is removed: 1 - pectineus muscle; 2 - long adductor muscle; 3 - thin muscle; 4 - adductor channel; 5 - vastus medialis; 6 - vastus intermedius; 7 - vastus lateralis muscle
And large lumbar(T. psoas major), originating from the XII thoracic and I-II lumbar vertebrae. Both muscles join together, pass under the inguinal ligament in the muscle lacuna and attach to the lesser trochanter of the femur.
Function: flexes the thigh and rotates it outward.
Innervation: lumbar plexus, L I -S II.
2.Psoas minor muscle(m. psoas minor) unstable, starts from the bodies of the XII thoracic and I lumbar vertebrae; attaches to the fascia iliaca.
Function: stretches the fascia iliaca. Innervation: lumbar plexus, L I -L II.
3.Piriformis muscle(m. piriformis) starts from the pelvic surface of the sacrum, passes through the greater sciatic foramen; attaches to the greater trochanter of the femur.
Function: rotates the thigh outward. Innervation: sacral plexus, S I -S II.
4.Obturator internus muscle(m. obturatorius internus) starts from the inner surface of the obturator membrane and the inner surface of the pelvic bone around the obturator foramen; attaches to the trochanteric fossa.
Function: rotates the thigh outward. Innervation: sacral plexus, L I -S II.
5.Superior and inferior gemellus muscles(mm. gemellus superior et inferior) start from the ischial spine (upper) and the ischial tuberosity (lower); are attached in the trochanteric fossa.
Function: rotate the thigh outward. Innervation: sacral plexus, L IV -S II
External pelvic muscles
1.Gluteus maximus muscle(m. gluteus maximus) starts from the outer surface of the ilium, from the dorsal surface of the sacrum and coccyx; attaches to the gluteal tuberosity of the femur.
Function: extends the hip, rotates outward, fixes the pelvis. Innervation: inferior gluteal nerve, L III -L IV.
2.Gluteus medius and minimus muscles(mm. gluteus medius et minimus) located under the gluteus maximus muscle. Start from the outer surface of the ilium; are attached to the greater trochanter of the femur.
Function: the thigh is abducted, the anterior bundles are rotated inward, the posterior bundles are rotated outward. With fixed lower extremities, tilt the pelvis to the side Innervation: superior gluteal nerve, L IV -S I
3.Tensor fascia lata(m. tensor fasciae latae) located on the outer surface of the thigh. It starts from the iliac crest, from the superior external iliac spine, goes down and passes into the fascia lata covering the thigh muscles.
Function: strains the fascia lata, flexes the hip and rotates it inward.
Innervation: superior gluteal nerve, L IV -S I
4.Quadratus femoris(m. quadratus femoris) starts from the ischial tuberosity; attaches to the intertrochanteric ridge.
Function: rotates the thigh outward. Innervation: sacral plexus, L IV -S I
5.Obturator externus muscle(m. obturatorius externus) starts from the outer surface of the pelvic bone, from the obturator membrane; attaches to the trochanteric fossa.
Function: rotates the thigh outward. Innervation: obturator nerve, L III -L IV.
Muscles of the free lower limb
Thigh muscles
There are 3 groups of muscles on the thigh: the anterior - extensor muscles, the posterior - flexor muscles and the medial - adductor muscles (see Fig. 68; Fig. 69 and 70).
Anterior group - extensor muscles
1. Quadriceps femoris(m. quadriceps femoris) located on the front surface of the thigh and consists of 4 heads - muscles. Rectus femoris muscle(m. rectus femoris) lies superficially on m. vastus intermedius; starts from the inferior anterior iliac spine; vastus medialis(m. vastus medialis) originates from the medial lip of the linea aspera, and vastus lateralis muscle(m. vastus lateralis)- from the lateral lip of the linea aspera; vastus intermedius(m. vastus intermedius) starts from the front surface of the thigh. In the distal part, all heads of the quadriceps femoris muscle pass into the common tendon surrounding the patella and are attached to the tibial tuberosity.

Rice. 69. Thigh muscles, front view (part of the muscle has been removed, others are cut and turned away): 1, 11 - pectineus muscles; 2-long adductor muscle; 3 - external obturator muscle; 4 - quadratus femoris muscle; 5 - adductor minimus; 6 - adductor magnus; 7 - vessels in the adductor canal; 8 - vastus intermedius;
9- long adductor muscle;
10- short adductor muscle
Function: extends the lower leg at the knee joint, flexes the thigh (only m. rectus femoris).
Innervation: femoral nerve, L II -L III
2. Sartorius(m. sartorius) starts from the superior anterior iliac spine; attaches to the medial surface of the tibial tuberosity.
Function: flexes the thigh and lower leg, rotates the limb bent at the knee joint inward.
Innervation: femoral nerve, L I -L II.

Rice. 70.Muscles of the lower limb, rear view:
a - superficial layer: 1 - tensor fascia lata; 2 - gluteus maximus muscle; 3 - biceps femoris muscle (long head); 4 - biceps femoris muscle (short head); 5 - plantaris muscle (vessels in the patellar fossa pass nearby); 6 - calf muscle; 7 - semimembranosus muscle; 8 - semitendinosus muscle; 9 - thin muscle; 10 - adductor magnus; b - part of the muscles is removed: 1 - gluteus medius; 2 - gluteus minimus; 3 - piriformis muscle; 4 - superior gemellus muscle; 5 - internal obturator muscle; 6 - inferior gemellus muscle; 7 - quadratus femoris muscle; 8 - gluteus maximus muscle; 9 - adductor magnus; 10 - short head of the biceps femoris muscle; 11 - popliteus muscle; 12 - soleus muscle; 13 - semitendinosus muscle; 14 - semimembranosus muscle; 15 - thin muscle; 16 - adductor magnus muscle
Posterior group - extensor muscles
1.Biceps femoris(m. biceps femoris) has two heads, occupies a lateral position. Short head (caput breve) originates from the distal part of the lateral lip of the linea aspera, long head (caput longum)- from the ischial tuberosity. Both heads form a common belly, which is attached to the head of the fibula.
Function: with a fixed pelvis, flexes the lower leg at the knee joint and extends the thigh.
2.Semitendinosus muscle(m. semitendinosus) located on the medial surface of the thigh. It starts from the ischial tuberosity, in the middle part it passes into a long tendon; attaches to the tibial tuberosity.
Function: with a fixed pelvis, flexes the lower leg and extends the thigh. Innervation: sciatic nerve, L V -S II.
3.Semimembranosus muscle(m. semimembranosus) starts from the ischial tuberosity with a lamellar tendon, which is half the length of the muscle; attaches to the medial condyle of the tibia.
Function: with a fixed pelvis, extends the thigh, bends and turns the lower leg inward.
Innervation: sciatic nerve, L IV -S I.
Medial group - adductor muscles
1.Pectineus muscle(m. pectineus).
2.Adductor longus muscle(m. adductor longus) starts from the superior branch of the pubic bone.
3.Thin muscle(m. gracilis).
4.Adductor brevis muscle(m. adductor brevis) originates from the lower branch of the pubic bone.
5.Adductor magnus muscle(m. adductor magnus) starts from the ischial tuberosity and the anterior surface of the lower branches of the ischium and pubis.
All of these muscles are attached to the medial lip of the linea aspera, and the gracilis muscle is attached to the tibial tuberosity.
Function: adduct and flex the thigh; the thin muscle flexes the lower leg and rotates it inward.
Innervation: obturator nerve, L II -L III.

Rice. 71.Calf muscles, front view: 1 - calf muscle; 2 - tibialis anterior muscle; 3 - soleus muscle; 4 - extensor pollicis longus; 5 - short extensor pollicis; 6 - extensor digitorum brevis; 7 - extensor digitorum longus; 8 - short peroneus muscle; 9 - peroneus longus muscle
Calf muscles
The lower leg muscles are divided into 3 groups: anterior, posterior and lateral (see Fig. 70; Fig. 71).
Front group
1. Tibialis anterior muscle(m. tibialis anterior) starts from the lateral condyle and the lateral surface of the tibia; attaches to the medial cuneiform bone and the base of the first metatarsal bone.
Function: extends and supinates the foot.
Innervation: deep peroneal nerve, L IV -S I.
2.Extensor digitorum longus(m. extensor digitorum longus) lies lateral to the previous muscle. It starts from the lateral condyle of the tibia, from the head of the fibula. The muscle is divided into 5 tendons, 4 of which are attached to the distal phalanges of the II-V fingers, the 5th to the V metatarsal bone.
Function: extends fingers and foot.
Innervation: deep peroneal nerve, L IV -S I
3.Extensor hallucis longus(m. extensor hallucis longus) starts from the lower part of the medial surface of the fibula; attaches to the distal phalanx of the first finger.
Function: extends the big toe, extends and supinates the foot. Innervation: deep peroneal nerve, L IV -S I
Back group
1.Triceps surae muscle(m. triceps surae) forms a surface layer. Comprises calf muscle(m. gastrocnemius), starting with two heads from the medial and lateral condyles of the femur, and soleus muscle(m. soleus), extending from the proximal bones of the leg. Both muscles combine to form a powerful calcaneal (Achilles) tendon(tendo calcaneus), attached to the calcaneal tubercle.
Function: flexes the foot and lower leg.
2.Plantaris muscle(m. plantaris) starts from the popliteal surface of the femur, passes into a long tendon, which is attached to the heel bone.
Function: pulls the knee joint capsule posteriorly. Innervation: tibial nerve, L V -S II
3.Hamstring muscle(m. popliteus) forms, together with subsequent ones, a deep layer. Originates from the lateral epicondyle of the femur; attaches to the proximal epiphysis of the tibia.
Function: bends the lower leg and rotates it inward. Innervation: tibial nerve, L V -S II
4.Flexor hallucis longus(m. flexor hallucis longus) begins on the posterior surface of the fibula and from the interosseous membrane, passes behind the medial malleolus; attaches to the distal phalanx of the first finger.
Function: bends the first finger.
Innervation: tibial nerve, L V -S II
5.Flexor digitorum longus(m. flexor digitorum longus) starts from the posterior surface of the tibia, passes behind the medial malleolus and at the sole is divided into 4 tendons, which are attached to the distal phalanges of the II-IV fingers.
Function: flexes the distal phalanges of the II-VI fingers, and also flexes and supinates the foot.
Innervation: tibial nerve, L V -S II
6.Tibialis posterior muscle(m. tibialis posterior) lies under the previous muscles. It starts from the proximal epiphyses of the bones of the leg, goes around the medial malleolus, and passes to the foot; attaches to the tuberosity of the scaphoid and three sphenoid bones.
Function: flexes and supinates the foot. Innervation: tibial nerve, L V -S II
Lateral group
1.Peroneus longus muscle(m. fibularis longus) starts from the head of the fibula; attaches to the medial sphenoid and first metatarsal bones.
Function: raises the lateral edge of the foot, simultaneously lowers the medial edge, flexes the foot.
2.Peroneus brevis muscle(m. fibularis brevis) starts from the fibula; attaches to the tuberosity of the metatarsal bone.
Function: flexes the foot, raises its lateral edge. Innervation: both muscles are innervated by the superficial peroneal nerve, L V -S II
Foot muscles
There are muscles of the rear and muscles of the sole of the foot. On dorsum of the foot There are two muscles: extensor digitorum brevis(m. extensor digitorum brevis) And extensor hallucis brevis
(m. extensor hallucis brevis). Both muscles start from the heel bone and attach to the phalanges of the I-V fingers. Function: extend fingers.
Innervation: deep peroneal nerve, L IV -S I On the sole muscles are divided into 3 groups (Fig. 72). The medial group consists of abductor hallux muscle(m. abductor
hallucis),flexor hallucis brevis(m. flexor hallucis brevis) And adductor hallucis muscle(m. adductor hallucis). The lateral group includes flexor of the little toe brevis(m. flexor digiti minimi brevis) And muscle that abducts the little toe(m. abductor digiti minimi). The middle group includes flexor digitorum brevis(m. flexor digitorum brevis),quadratus plantaris(m. quadratus plantae),lumbrical muscles(mm. lumbricales),plantar interosseous muscles(mm. interossei plantares) And dorsal interosseous muscles(mm. interossei dorsales).
Function: the lumbrical muscles flex the phalanges of the fingers, the interosseous dorsal muscles move apart, and the interosseous plantar muscles move the fingers.
Innervation: medial and lateral plantar nerves, L V -S II

Rice. 72. Muscles of the foot, plantar side:
1 - muscle that abducts the little toe; 2 - plantar interosseous muscles; 3 - short flexor of the little toe; 4 - flexor digitorum longus tendon; 5 - tendons of the short flexor of the fingers; 6 - fibrous sheaths of the toes; 7 - lumbrical muscles;
8 - short flexor of the big toe;
9- tendon of the long flexor of the big toe; 10 - flexor digitorum brevis;
11 - muscle that abducts the big toe; 12 - plantar aponeurosis (cut off); 13 - calcaneal tubercle
Fascia of the lower limb
In the pelvic cavity fascia iliaca(fascia iliaca) covers the iliopsoas muscle and is part of the intra-abdominal fascia. In the medial direction it forms the iliopectineal arch (arcus iliopectineus), delimiting 2 spaces under the inguinal ligament - the lateral muscular lacuna (lacuna m usculorum)(for the femoral nerve), and medial vascular lacuna (lacuna vasorum)(for femoral vessels).
Proprietary fascia of the thigh - fascia lata(fascia lata), giving off spurs to the rough line of the femur, it forms two intermuscular septa of the thigh: lateral (septum intermuscular femoris laterals) and medial (septum intermusculare femoris mediale). Between the intermuscular septa and the femur there are 3 osteofibrous vagina muscles of the anterior, posterior and medial groups.
Under the inguinal ligament, the fascia lata splits into 2 layers - superficial and deep. Superficial leaf fascia lata forms the subcutaneous fissure (hiatus saphenus), bounded by a crescent-shaped edge (margo falciformis) and closed cribriform fascia(fascia cribrosa). Vessels and nerves pass through this gap. The subcutaneous fissure is the external opening femoral canal. deep leaf covers the fascia lata m. pectineus.
Fascia of the leg(fascia cruris)- continuation of the fascia lata, gives two to the fibula intermuscular septum of the leg: front (septum intermusculare anterius cruris), separating the peroneal muscles from the extensors, and the posterior (septum intermusculare posterius), separating the extensors from the flexors. As a result, 3 osteofibrous muscle sheaths are formed on the lower leg front, back And lateral groups.
In the distal part of the leg, the fascia in front thickens and forms two ligaments: upper And inferior extensor tendon retinaculum(retinaculi mm. extensorum superius et inferius). The tendons of the muscles of the anterior group of the lower leg pass under them. The septa extending from the inferior retinaculum of the extensor tendons divide the space under the ligament into 4 osteo-fibrous canals: 3 tendon and 1 vascular. IN lateral canal the tendon passes m. extensor digitorum longus, average - m. extensor hallucis longus, in the medial - m. tibialis anterior.
Between the medial malleolus and the calcaneus there is a strong ligament - the retinaculum of the flexor tendons (retinaculum musculorum
flexorum). The septa extend deeper from the ligament, forming 3 osteofibrous canal. Behind the medial malleolus is the tibialis posterior tendon, posterior to it is the flexor digitorum longus tendon, and deeper is the flexor hallucis longus tendon.
From the lateral malleolus to the calcaneus extend superior and inferior peroneal retinaculum(retinaculi musculorum fibularium superius et inferius), under which the tendons of the peroneal muscles pass.
Dorsal fascia of the foot(fascia dorsalis pedis) thin, fuses with the bones of the metatarsus, forms superficial and deep layers, between which the tendons of the extensor muscles pass. On the plantar side there is a well-defined fascial thickening - plantar aponeurosis(aponeurosis plantaris). The medial and lateral intermuscular septa extend from it to the bones of the foot, forming 3 osteofascial sheaths corresponding to 3 muscle groups.
Elements of the topography of the lower limb
The piriformis muscle, passing through the greater sciatic foramen, divides it into 2 openings: suppiriformis (for. suprapiriforme) and infrapiriform (for. infrapiriforme). The superior gluteal artery, vein and nerve of the same name pass through the first, the pudendal nerve, pudendal artery and vein, sciatic nerve and posterior cutaneous nerve of the thigh, as well as the inferior gluteal nerves, artery and vein pass through the second.
The pelvic cavity communicates with the anteromedial surface of the thigh obturator canal(canalis obturatorius), the walls of which are formed by the pubic bone and the upper edges of both obturator muscles. The canal has 2 openings: internal and external, through which the vessels and nerves of the same name pass.
In the upper third of the thigh on its anterior surface there is femoral triangle(trigonum femorale), bounded superiorly by the inguinal ligament, laterally by the sartorius muscle and medially by the adductor longus muscle. In the femoral triangle is femoral canal(canalis femoralis)(Fig. 73), which does not exist normally, but occurs with femoral hernias. The channel has 3 walls: lateral- femoral vein, rear- deep layer of fascia lata, front- its superficial leaf, and two holes: internal - femoral ring (anulus femoralis), located in the medial corner

Rice. 73. Elements of the topography of the right groin area and lower limb (photo from the specimen):
1 - anterior superior iliac spine; 2, 3 - aponeurosis of the external oblique abdominal muscle; 4 - rectus abdominis muscle; 5 - superficial epigastric vein; 6 - superficial ring of the inguinal canal; 7 - round ligament of the uterus passing through it; 8 - pubis; 9 - thin muscle; 10 - long adductor muscle; 11 - pectineus muscle; 12 - great saphenous vein; 13 - vessels to the external genitalia; 14, 16 - fascia lata; 15 - accessory saphenous vein; 17 - position of the femoral canal; 18 - femoral vein; 19 - inguinal ligament; 20 - femoral artery; 21 - femoral nerve; 22, 23 - nerves to muscles; 24 - sartorius muscle; 25 - superficial vessels; 26 - tensor fascia lata
Rice. 74. Adductor muscles of the thigh, right, view from the medial side:
1- adductor magnus; 2 - semitendinosus muscle; 3 - adductor channel; 4 - semimembranosus muscle;
5- vastus medialis muscle;
6- intermuscular septum; 7 - rectus femoris muscle; 8 - long adductor muscle; 9 - short adductor muscle; 10 - pectineus muscle;
11 - obturator membrane; 12 - iliacus muscle; 13 - psoas major muscle; 14 - piriformis muscle; 15 - sacrospinous ligament
vascular lacuna, limited anteriorly by the inguinal ligament, posteriorly - lig. iliopectineum medially - lacunar ligament(place of attachment of the inguinal ligament to the pubic bone), laterally - by the femoral vein, and externally - by the saphenous fissure (hiatus saphenus). In the lower third of the thigh is determined adductor canal(canalis adductorius)(Fig. 74),
going into the popliteal fossa. The canal is formed medially by the adductor magnus muscle, laterally by the vastus medialis muscle, and anteriorly by the broad adductor intermuscular septum. (septum intermusculare vastoadductorium). The canal contains the femoral vessels and the saphenous nerve.
Popliteal fossa(fossa poplitea) contains the vessels of the same name, the sciatic nerve and its branches, lymphatic vessels and nodes. The fossa is formed from above and medially by the tendons of the semimembranosus and semitendinosus muscles, from above and laterally by the tendon of the biceps femoris muscle, below and from the inside by the medial head of the gastrocnemius muscle, below and from the outside by the lateral head of the same muscle. The popliteal fossa passes down into ankle-popliteal canal(canalis cruropopliteus), passing along the back surface of the lower leg, between the superficial and deep layers of the lower leg muscles. The canal contains the posterior tibial artery, vein and nerve. Branches from the ankle-popliteal canal inferior musculofibular canal(canalis musculoperoneus inferior), lying between the fibula, flexor hallucis longus and tibialis posterior. The medial and lateral plantar grooves run along the sole (suici plantares medialis et lateralis), which are located on the sides of m. flexor digitorum brevis.
Questions for self-control
1.Indicate the origin, insertion and function of the internal pelvic muscles.
2.Indicate the origin, insertion and function of the external pelvic muscles.
3.What groups are the thigh muscles divided into? Indicate the origin, insertion, and function of each muscle group.
4.What groups are the lower leg muscles divided into? Indicate the origin, insertion, and function of each muscle group.
5.Name the muscles of the foot by group. What function do they perform?
6.What fascia of the lower limb do you know? What do they form (lining)?
7.What are the walls and openings of the femoral canal formed by?
8.What is the adductor canal formed by? What's going on in it?
9.What is the ankle-popliteal canal formed by?
BRIEF INFORMATION ABOUT THE MUSCLES OF THE HEAD AND NECK
Head muscles are divided into two main groups: facial muscles(m. faciei) And masticatory muscles(mm. masticatorii). Other muscle groups: the external muscles of the eyeball, the muscles of the auditory ossicles, the muscles of the tongue, the muscles of the soft palate and pharynx are considered along with other organ systems.
The facial muscles (Fig. 75) are thin muscle bundles that start from the bones of the skull and are attached to the skin or lie entirely in soft tissues. When they contract, they move the skin of the face, which is called facial expressions(previously these muscles were designated as facial).
The most significant of the muscles of this group, located on the cranial vault, is supracranial muscle(m. epicranius). It has two bellies made of muscle tissue - the frontal and the occipital, between which there is a wide and flat tendon - the tendon helmet. When contracted, it gathers the skin of the forehead into transverse folds.
The muscles surrounding the palpebral fissure include orbicularis oculi muscle(m. orbicularis oculi), which closes the palpebral fissure; corrugator muscle(m. corrugator supercilii), And depressor brow muscle(m. depressor supercilii), and proud muscle(m. procerus), lowering the skin of the glabella down.
Near the nasal openings are located nasal muscle(m. nasalis), narrowing the nasal openings, and depressor septum muscle(m. depressor septi nasi).
The largest number of facial muscles are grouped around the mouth. This orbicularis oris muscle(m. orbicularis oris), which partially lies in the thickness of the lips, when contracting, pulls them forward and narrows the oral fissure; levator labii superioris muscle(m. levator labii superioris);levator anguli oris muscle(m. levator anguli oris);depressor labii muscle(m. depressor labii inferioris);depressor anguli oris muscle(m. depressor anguli oris). In addition, pull the corner of the mouth up big And zygomatic minor muscles(m.m. zygomaticus major et minor), and laterally - laughter muscle(m. risorius) And buccal muscle(m. buccinator).
Chewing muscles, paired, larger and stronger than the facial muscles, produce movement of the lower jaw in the temporomandibular

Rice. 75. Facial muscles:
1 - frontal belly of the supracranial muscle; 2 - tendon helmet; 3 - occipital belly of the supracranial muscle; 4 - subcutaneous muscle of the neck; 5 - muscle that lowers the angle of the mouth; 6 - muscle of laughter; 7 - muscle that lowers the lower lip; 8 - orbicularis oris muscle; 9 - zygomaticus major muscle; 10 - zygomatic minor muscle;
11 - muscle that lowers the nasal septum; 12 - muscle that lifts the upper lip; 13 - nasal muscle; 14 - circular muscle of the eye; 15 - muscle of the proud
jaw joint (Fig. 76). These include masseter muscle(m. masseter),temporal muscle(m. temporalis) And medial pterygoid muscle(m. pterygoideus medialis), which, with bilateral contraction, raise the lower jaw, as well as lateral pterygoid muscle
(m. pterygoideus lateralis), with bilateral contraction, it moves the jaw forward. If a particular muscle contracts on only one side (unilateral contraction), the jaw will move to the side.
neck muscles, paired, arranged in several layers (Fig. 77). The most superficial lies subcutaneous muscle of the neck(platysma), tightening the skin of the neck, and sternocleidomastoid muscle(m. sternocleidomastoideus), with bilateral contraction, throwing back the head.
The middle group consists suprahyoid And sublingual muscles. The first include digastric(m. digastricus),mylohyoid muscle(m. mylohyoideus),geniohyoid muscle(m. geniohyoideus), lowering the lower jaw, as well as stylohyoid muscle(m. stylohyoideus), moving the hyoid bone. The suprahyoid muscles form the lower wall of the oral cavity - the diaphragm of the mouth.
The infrahyoid muscles pull the hyoid bone down. These include omohyoid muscle(m. omohyoideus),sternohyoid muscle(m. sternohyoideus),sternothyroid and thyrohyoid muscles.
Deeper than the middle group lie the deep muscles of the neck. Among them it should be noted front, middle And posterior scalene muscles,(m.m. scalenus anterior, medius et posterior) with bilateral contraction, flexion of the cervical spine, as well as long neck muscles And heads(m.m. longus colli et capitis), also tilting the neck and head forward, respectively. At the top there is another muscle group - suboccipital muscles, providing head movement.
Fascia of the head and neck
The facial muscles, with the exception of the buccal muscle, are not covered by fascia. The most well-formed fascia of the head is chewable And temporal, covering the muscles of the same name.

Rice. 76. Chewing muscles and some facial muscles:
a - left view: 1 - temporalis muscle with temporalis fascia; 2 - buccal muscle with the duct of the parotid salivary gland passing through it; 3 - orbicularis oris muscle; 4 - muscle that lowers the lower lip; 5 - muscle that lowers the angle of the mouth; 6 - chewing muscle; 7 - muscle that lifts the upper lip; 8 - zygomaticus major muscle; 9 - zygomatic minor muscle;
b - bottom view of the skull: 1 - cavity of the temporomandibular joint with an articular disc; 2 - lateral pterygoid muscle; 3 - medial pterygoid muscle

Rice. 77. Neck muscles:
1 - stylohyoid muscle; 2 - mylohyoid muscle; 3 - digastric muscle; 4 - thyrohyoid muscle; 5, 8 - omohyoid muscle; 6 - sternohyoid muscle; 7 - sternocleidomastoid muscle; 9 - scalene muscles
On the neck according to V.N. Shevkunenko distinguishes 5 fasciae, described in detail in the 2nd volume in the section “Muscles and fascia of the neck”. In modern International Anatomical Terminology, only 3 are fixed records(superficial, pretracheal and prevertebral) neck fascia, corresponding to three of the five fascia of the neck according to V.N. Shevkunenko. The first covers the sternocleidomastoid and suprahyoid muscles, the second covers the sublingual muscles, and the third covers the deep muscles of the neck.
Back pain can be associated with many health problems, such as a spinal disc injury. Recently, another disease has become widespread, which has attracted great attention from doctors - pain in the area where the thoracolumbar fascia is located.
It is important to pay attention to this problem in time in order to be able to prevent many diseases that can definitely ruin a person’s full life. Basically, special attention should be paid to strengthening the back muscles.
What is fascia?
Fascia is a thick connective tissue that covers muscles and bones, but its most important job is to support all organs. Sometimes there may be pain in this area. As soon as back pain appears, it can be assumed that problems have begun in the fascia area. In this case, it is important to establish the cause, and there may be many of them.
What types of pain are there?
Not long ago, laboratory studies were carried out by scientists who came to the conclusion that pain can occur in three types:
- Sometimes the deep plate of the thoracolumbar fascia is subjected to minor trauma or inflammation, in which case active stimulation of the nerve endings occurs. The fascia in the thoracolumbar region is very close to the skin. During the inflammatory process, all nerve impulses are sent to the brain, and pain occurs.
- If a person is injured, the tissues can become stiff and overloaded. These changes negatively affect the body's posture and mobility, causing not only discomfort but also pain over time.
- Any injury irritates the nerve endings. The nerves branch, and the root itself is located in the spinal cord. The injury causes pain in a specific area of the back.

Layers of fascia
The thoracolumbar fascia is divided into 3 main layers. Almost all the muscles in the back are attached to the fascia. The entire muscle group runs from the first longitudinal vertebra to the very bottom:
1. The layer that is located at the back starts from the twelfth vertebra and stretches to the very bottom. Along the way, this layer has the internal oblique muscle and the abdominal muscle. In this case, the fascia connects the muscles of the back and the peritoneum.
2. The middle layer is the broad dorsi muscle; it acts as a support for the body and helps to move the body weight freely. This layer begins directly from the thoracolumbar fascia.
3. The front layer helps to bend the body and calmly hold any upright posture.

Oddly enough, back pain can occur not only in adults, but even in the youngest. Intense pain can lead to a person’s disability.
Main functions of fascia
It is worth noting that fascia is primarily an inelastic support that allows you to properly hold the pelvis, torso and all limbs, and also allows you to freely distribute the entire load throughout the body. Let us consider in detail what functions the lumbothoracic fascia performs:
- While the muscles in the abdomen begin to activate, the fascia begins to restrict the movement of the pelvic bones, and the work of the iliac joints improves.
- When horizontal muscle tension occurs, the transverse abdominal muscles begin to contract in the peritoneum and thereby stabilize the pelvis.
- The muscles that are connected to the fascia allow you to balance tension and force the group of muscles that are responsible for this to straighten the spine.
Most often, pain occurs in the lower back.
Fascia and its structure
Latin is often used in medicine. The thoracolumbar fascia is called fascia thoracolumbalis. In fact, the fascia itself is similar to a special depression where the spinal muscles are located. If we look at it in more detail, it resembles two leaves; they can be divided into back and front. The anterior leaf is located in the lumbar region and stretches between the processes of the vertebra. The superficial plate of the thoracolumbar fascia begins on the processes of the vertebrae and is attached to the ribs at the corners.
Is it worth pumping up your back muscles? How to do this correctly?

It is important to remember all the rules that exist for these exercises:
1. First of all, it is worth considering that classes should be held regularly. You can conduct such classes twice a week, but you shouldn’t try too hard either. If you do such exercises too often, the muscles will not have time to recover.
2. You should not perform all the exercises at once; it is advisable to do several approaches. Each exercise is done 15 times.
3. Under no circumstances should you start exercises without warming up your muscles.
4. Complexes must change, otherwise the muscles will get used to such constant loads.
Many people are interested in what to do if the thoracolumbar fascia is weak. How to pump it up to forget about back pain? All the recommendations given above will help cope with this problem.
A set of exercises to strengthen the back muscles
Let's look at a few exercises that will help strengthen your back muscles:

- After the body is slightly warmed up, you can begin the first exercise. The body is lowered to a position parallel to the floor, the legs are slightly bent at the knees, and the person holds dumbbells in his hands. The dumbbells should be raised in your hands so that your shoulder blades meet on your back. Such exercises are performed slowly, because the main effect is stretching the latissimus muscles.
- If you need to strengthen the area where the thoracolumbar fascia is located, the exercise should be selected as a pull-up. It is performed on the horizontal bar. Place your hands shoulder-width apart, stretch up to the bar, trying to reach it with your chin, after which the body slowly lowers down.
- For the next exercise, you can use a bench. You need to stand with your back to it and gradually lean to the right, leaning on the bench with your right hand. It is important to bend your lower back well. The left leg bends at the knee, and the right acts as a support. To properly strengthen the thoracolumbar fascia, this exercise can be made more difficult. For example, take dumbbells in your left hand and stretch up with your right hand. Next, change hands and do the same with your left hand, dumbbells in your right hand.
- To perform this exercise, you will need to use a hard mat on which to place your pelvis and legs. A person must lie down with his pelvis and legs, while his legs must be fixed in any way, just so that they do not move. Hands are placed on the back of the head. The main task is to raise your body as much as possible in this position, and then slowly lower it down. It is important to bend your back, jerking is prohibited, everything is done smoothly.

Such seemingly simple exercises will help relieve back pain and significantly strengthen muscles, which is important for a person’s normal, active lifestyle.
What should you consider when training at home?
To strengthen the lumbothoracic fascia, you should always remember the main rules when performing exercises:

If you follow all the recommendations given in the article, you can get rid of such a problem as back pain once and for all. Additionally, you can consult with a doctor - a specialist who can not only help you create a diet for the day, but also select the right exercises.
Scientists believe that any pathological changes in the functioning of the musculoskeletal system are people’s retribution for walking upright. Throughout life, our body experiences enormous stress, as a result of which ligaments, tendons and cartilage suffer. When joints are healthy, they operate smoothly and quietly. But sometimes during movement there is a crunching sound in the bone joints, especially large ones. In most cases, it is accompanied by discomfort and pain. Why does the hip joint crunch, what to do about it - such questions are of great concern to those suffering.
Prerequisites for functional changes
The hip joint is the junction of the largest bones: the femur and the pelvis. It consists of the head, the acetabulum, along the edge of which the acetabular lip is located, and the articular space. The cavity of the joint is filled with synovial fluid and lined with cartilage tissue, which provides it with high-quality gliding. The acetabular lip covers the head and securely fixes it, preventing it from falling out of the acetabulum. If the integrity of any of these components is violated, the hip joints crack. In medicine, this problem is called snapping hip syndrome.

The reasons for this condition are different. Sometimes the presence of such symptoms occurs without any prerequisites and is not a sign of illness. Factors causing degenerative changes in the structure of cartilage:
- excessive physical activity;
- salt deposition as a consequence of disturbed water-salt and mineral balance;
- mechanical trauma that causes a violation of the integrity of the bone and cartilaginous structures of the joint;
- increased flexibility of bone joints;
- immaturity of the muscular and connective apparatus around the joint.
Other causes of crunching in the hip joint are associated with degenerative changes resulting from the following factors:
- development of arthritis or arthrosis;
- gout or progressive osteochondrosis;
- inflammatory processes in cartilage, tendons and other elements of the ligamentous apparatus;
- increased degree of wear of articular surfaces;
- overweight;
- mismatch of bone joint surfaces.
Sometimes crunching and clicking sounds are associated with metabolic and endocrine disorders, poor nutrition and non-compliance with the daily routine.
Such functional changes cannot be attributed only to the age factor, because sometimes a crunch in the hip joint occurs in a child. Prerequisites: congenital pathologies, underdevelopment of muscle tissue around ligaments and cartilage, trauma.
Symptoms of pathology
During its operation, the bone joint undergoes heavy loads, which entails negative consequences that have a destructive effect on its tissues. The very first sign of functional disorders is a crunch in the hip joint without pain.
A characteristic sound signals wear of bone joints or the beginning of the development of destructive changes in tissues. Depending on the extent of the spread of this process, a clicking hip is accompanied by pain of varying degrees of intensity, discomfort, and limited mobility.
In the problem area, a feeling of springy resistance may appear, reinforced by the subsequent failure of the head. Such clicks are characterized by the onset of the development of arthrosis or polyarthritis. The patient experiences swelling and swelling of the tissues surrounding the joint, and the body temperature rises.
Classification of pathological disorders
Clicking and crunching sounds in the thigh are classified depending on the location of the problem:
- outer. The sound characteristic of pathology occurs in the outer part of the femoral diarthrosis due to the jumping off of the connective fascia when moving from the greater trochanter of the femur. Having undergone systematic blows, the joint capsule becomes inflamed, and the patient develops bursitis;
- intra-articular. This species is characterized by disturbances inside the diarthrosis cavity. As a result of deterioration in the sliding of the head along the acetabulum, it jumps off, making a sound similar to a click. An example of an intra-articular pathology is congenital dysplasia;
- interior. The mechanism of the crunch is caused by the rolling of the iliopsoas muscle through the head of the femoral bone. If left untreated, the risk of bursitis complications increases significantly.
Types of pathologies
A characteristic sign does not always indicate a problem. Clicking sounds can occur due to the accumulation of air bubbles in the synovial fluid, during excessive exercise or due to stress. However, if they worsen the quality of life, continue for a long time and are accompanied by other signs, then the person needs the help of a specialist.
To understand why the hip joint crunches, it is necessary to carefully examine the symptoms of the pathology and determine its type. Even if this is the only visible sign of pathology, examination may reveal accompanying symptoms, allowing a correct diagnosis to be made and treatment to begin.
Iliopsoas syndrome
The iliopsoas muscle is the most common cause of clicking joints. This is explained by the tendon jumping over the acetabular labrum and femoral head during excessive and intense physical activity. At first, sounds characteristic of the problem occur rarely, but as the disorder progresses, their frequency increases and becomes almost constant. Gradually, other signs join the characteristic crunch:
- dull pain in the groin when flexing and straightening the limbs;
- feeling of resistance in the joint;
- joint weakness.

A special test is performed for diagnosis. This muscle is loaded with various sets of exercises. If characteristic sounds occur during their execution, the patient’s diagnosis is confirmed.
Systematic friction of the ligaments can cause iliopectineal bursitis, which significantly complicates the patient’s condition.
Iliotibial band syndrome
If the hip joint is cracking, a possible cause is increased friction in the iliotibial fascia. This type of pathology is most common in athletes whose occupation is associated with intense mobility of the limbs. Characteristic sounds are accompanied by pain on the outside of the joint. Possible complications include trochanteritis, an inflammatory process that develops in the trochanteric bursa. It is characterized by increased pain in the periarticular area, redness of the tissues and their swelling.
More details

Acetabular labral tear
The cartilaginous lip is involved in stabilizing the hip joint. Violation of its integrity occurs due to injury or degenerative changes in the structure of tissues. The rupture is characterized by:
- pain in the groin area or above;
- characteristic sounds when moving;
- impaired mobility;
- feeling of resistance in the joint.

For diagnosis, the patient is subjected to a special test with physical stress on the bone connection. Pathology is indicated by the appearance of a painful crunching sound.
Osteoarthritis
Degenerative changes in the structure of cartilage and ligaments often cause a person to have cracking hip joints. One of the pathologies is osteoarthritis. It is more often diagnosed in the male half of the population, since they are more susceptible to heavy physical activity and sports. The following signs indicate the disease:
- restriction of mobility in the problem area;
- sensation of joint friction;
- “starting” pain syndrome (when the first steps after a long period of rest are difficult);
- visible deformation of the bone connection (in advanced forms).

Pain occurs not only while walking, but when supporting the damaged tendon. If the disease has become advanced, the feeling of discomfort persists even at rest. If left untreated, the patient faces disability.
Osteochondropathy
If a crunch occurs in the hip joint in a child, then it can be assumed that he has Perthes disease or osteochondropathy. Usually occurs in children under 12 years of age. The essence of the pathology is necrotic processes of the femoral head, accompanied by the following symptoms:
- pain syndrome;
- fatigue when walking;
- limited limb mobility;
- limping gait;
- shortening of one leg.
Without treatment, the disease progresses rapidly and leads to deforming osteoarthritis.
Mechanical damage
Joint injuries occupy a wide niche in the development of pathological disorders in humans. A characteristic crunch can accompany sprains and ruptures of ligaments and tendons, dislocations, fractures, and bruises. The patient experiences pain of varying degrees of intensity depending on the type of injury received, swelling and swelling of soft tissues, bruising, and limited mobility.
Hip dysplasia
This type of joint pathology is more typical for newborns and is diagnosed by an orthopedist in the patient’s infancy. If left untreated at a later age, the crunching and clicking sounds are accompanied by lameness, “duck gait,” a feeling of heaviness, fatigue in the hip, and instability of the joint. In the future, dysplasia can develop into coxarthrosis.

For any functional disorders accompanied by a crunch of the hip joint, differential diagnosis is necessary.
Crunching in the femoral joint with pain also occurs in other diseases: intervertebral hernia, cartilage tear, fracture of the pelvic bones or femoral neck, osteoperiostitis of the pubic bone and others.
Diagnosis of pathology
It is naive to believe that cracking joints are harmless manifestations of functional changes in bone structures. Such symptoms can mask serious pathologies that require timely assistance from a specialist.
Despite the possibility of making a preliminary diagnosis using special tests and samples, final conclusions about the patient’s condition can only be obtained by conducting additional types of examination. These include:
- ultrasonography;
- radiography;

The doctor decides which one to choose, based on the results of the preliminary examination and the technical capabilities of the medical institution. When the results of additional tests are ready, a consultation with an orthopedic traumatologist will be required.
Treatment methods
When your hip joints are cracking, you should never let the problem take its course. No, it won’t go away on its own, but complications will definitely appear. The choice of treatment method depends on the nature of the pathology. Therapeutic manipulations with crunchy joints are carried out in two directions: conservative and surgical.
Conservative therapy
From the beginning of treatment, conservative medicine is used. If you are not in a hurry to see a specialist because you are afraid of a scalpel, then you don’t have to worry, no one will operate on you right away.
First of all, the patient will be asked to review the load regime on the limb and, if possible, unload it as much as possible. If the pathology is inflammatory in nature, non-steroidal anti-inflammatory drugs are prescribed. They allow you to level out tissue damage and eliminate pain. These include Nimesulide, Celebrex, Ketanov, Ibuprofen, Piroxicam and others. They are fast-acting, have a symptomatic effect, but can cause adverse reactions. You cannot use such products for a long time, as their effectiveness decreases.

To alleviate the patient's condition, he is prescribed glucocorticosteroid hormonal drugs. The most popular are Hydrocortisone, Diprospan, Kenalog. If the disease is complicated by severe pain, then injections of glucocorticosteroids are administered into the area of the joint capsule. These are hormonal drugs that ensure normal blood flow in tissues, reduce muscle spasms, and eliminate pain.
To reduce pain and muscle spasms, the doctor may recommend taking muscle relaxants (Mydocalm, Sirdalud). Warming ointments are prescribed for the same purpose. They do not have a pronounced therapeutic effect, but relieve pain well. The most common are Espol, Menovazin, Nicoflex-cream, Gevkamen, Finalgon.

For arthrosis, chondroprotectors are used to restore cartilage tissue and synthesize synovial fluid inside the joint. Their action is aimed at preventing destructive changes. The disadvantage is the need for long-term use, since the drug has a cumulative effect. When treating crunching and clicking, Glucosamine, Teraflex and Chondroitin sulfate are used. If synovial fluid is formed in insufficient quantities, injections with hyaluronic acid are injected into the diseased joint to replace it. Examples of such agents are Ostenil, Farmatron, Durolan and others.
At the first manifestations of a pathological disorder of the bone articulation, accompanied by characteristic clicks, you should consult a doctor. The sooner the correct diagnosis is made, the greater the chances of a favorable outcome of therapy. However, the disease is treated not only with medication.
Physiotherapy
Exercise therapy has a good therapeutic effect for any problems with cartilage and ligaments. The set of exercises is aimed at strengthening muscle tissue in the periarticular area, ligaments and mobile joints, restoring motor functions and improving the support functions of the limb.
You need to practice regularly and always in the presence of an instructor who monitors and corrects the correct execution of the complex. When doing exercise therapy, no additional loads should be placed on the affected joint that could aggravate the patient’s condition.
For people suffering from snapping hip syndrome, doctors advise monitoring their physical activity, minimizing any sports training during treatment, or completely abandoning it for a while. If you cannot fully comply with these conditions, then it is better to replace them with swimming.
Physiotherapy
The use of a physiotherapeutic set of procedures allows you to reduce the intensity of discomfort and completely get rid of crunching, clicking and pain. Some types are used even after surgical treatment to reduce soft tissue swelling. Regeneration will be much more efficient.
Depending on the root cause of the pathology and the diagnosis, physiotherapeutic methods for treating clicking in the joints include:
- electrical stimulation;
- cryotherapy;
- acupuncture;
- electrophoresis;
- magnetic therapy;
- laser correction;
- shock wave therapy.
The great advantage of this type of treatment is that they allow you to act on the affected area without affecting nearby tissues and structures. Using these techniques, you can significantly reduce the dosage of medications taken without compromising the effectiveness of therapy. Massage as part of a complex treatment for cracking in the hip joint without pain also gives a good result.
Treatment of joints Read more >>
Proper nutrition
When dealing with clicking and crunching in bone joints, nutrition is important. The patient's diet should be complete, balanced, and help reduce body weight. The diet should include fatty fish, mainly sea fish, dairy products, poultry, legumes, nuts, other protein-rich foods, fruits and fresh vegetables. If you have problems with cartilage and bone joints, it is useful to eat gelatin (aspic, jellied meat, jelly). Sweets such as marshmallows and marshmallows are allowed, but you should not overuse them.
During treatment, you should avoid nightshade vegetables, red meat, preservatives and smoked foods. Alcohol in any form or quantity is strictly prohibited. When planning your diet, you need to reduce your salt intake.
Surgery
If the use of medications does not achieve the desired result, this may be a reason for surgical treatment. With internal and external localization of the problem, we can limit ourselves to partial intersection of the tendon of the iliopsoas muscle at the place of its attachment to the joint. If the localization of the pathology is intra-articular, then a complete replacement of the bone joint will be required.

With timely medical care for hip crunch, you can get rid of the problem only with conservative treatment without surgery.
Crunching in the hip joint cannot be considered a disease. This is one of the signs of any of the known pathologies of the musculoskeletal system. If it appears, it means that there is a malfunction in the body and it needs medical attention. You should not hope for a miracle and quick healing, because the problem can be dealt with with conservative treatment. If you let the situation take its course, the operation cannot be avoided.
The lumbosacral spine: how it works, main diseases
The spine is a very complex skeletal system that serves as the supporting axis of the body and ensures upright posture. It reliably protects the spinal cord and ensures the correct location and functioning of internal organs. It is to this that all parts of the skeleton are attached.
The spine also provides static stability and dynamic mobility of the human body. It consists of several departments. Each of them has its own structural features and functions. One of these sections, which experiences enormous loads every day, is commonly called the lumbosacral spine.
General information about the department
As in other sections, there are vertebrae in the lumbosacral spine. Each vertebra has anterior and posterior sections. The anterior section is the vertebral body, the structure of which is designed for easy folding of the vertebrae into a vertical structure.
The bodies bear the main weight and resist compression. The posterior section is an arch that protects the spinal cord. In addition, it serves to connect the spinal motion segments. Behind the arch there are processes that serve to attach ligaments and muscles.
Each vertebra has 4 facet joints, with the help of which it is connected to neighboring vertebrae. These joints provide mobility to the spinal column.
As a result of the placement of the vertebrae one above the other, the arches form a hollow tube called the spinal canal. This is where the spinal cord coming from the brain is located. Nerve fibers diverge from it in all directions. They form the roots of the spinal nerves. The spinal cord ends at the level of the 2nd lumbar vertebra. The roots extending from it hang further into the spinal canal and exit through the intervertebral foramina.
Between the vertebral bodies there are intervertebral discs, which serve to unite the vertebrae and eliminate friction between them. They look like a ring with a jelly-like substance in the center (core). The disc annulus consists of elastic fibrous fibers that are attached to the vertebral bodies. These discs also perform a shock-absorbing function during human movement, ensuring the sliding of the vertebrae.
With spinal injuries or frequent spinal overstrains, the liquid core may leak through cracks in the annulus fibrosus. In this case, intervertebral hernias are formed, which pinch the nerve roots and cause pain.
Thus, the anterior complex of the spine acts as a support for the entire body, and the posterior complex protects the spinal cord, controls the mobility of the vertebrae and fastens the spinal motion segments.
Spinal motion segment
The spinal motion segment is the part of the spine that is formed by 2 adjacent vertebrae. It also includes the ligamentous apparatus of these vertebrae, their joints, intervertebral disc and paravertebral muscles. Each such segment has 2 intervertebral foramina, through which blood vessels and spinal nerve roots pass.
The lumbar region contains 5 such spinal motion segments. In this case, the last segment is formed by the 5th lumbar and 1st sacral vertebrae.
Lumbar spine
This part of the spine consists of 5 vertebrae. In some cases, during lumbarization, there are 6 vertebrae in it, which is a variant of the norm. The vertebrae of this section are designated by the Latin letter L and a number corresponding to the serial number of the vertebra.
 It is the lumbar region that bears the entire weight of the overlying spine. Because of this, the vertebrae have their own characteristics. All of them have a large support part, which increases from L1 to L5. Not only the width, but also the height of the vertebral body increases.
It is the lumbar region that bears the entire weight of the overlying spine. Because of this, the vertebrae have their own characteristics. All of them have a large support part, which increases from L1 to L5. Not only the width, but also the height of the vertebral body increases.
The lumbar vertebrae have the most pronounced and massive processes. The central parts of the transverse processes are rudiments of ribs that merged with the true transverse processes during evolution. At the base of these processes there are also small additional processes.
The spinous processes are located almost horizontally posteriorly, almost at the level of the vertebral bodies. Their ends are thickened and directed backwards. This location and structure of these processes is associated with great mobility of the spine in this part.
The L5 vertebra should be highlighted separately. Its body is higher in front than in the back and has a wedge shape. This structure is necessary for the formation of lumbar lordosis.
Despite the fact that the intervertebral foramina in this part of the spine are quite wide, it is here that pain syndrome is most often observed due to damage to the roots. This is explained by the high mobility of the department and the heavy loads on it. The exception is the 5th vertebra. It is he who has the smallest intervertebral foramen at the junction with the sacrum, despite the fact that the corresponding spinal nerve has the largest diameter among all spinal nerves.
Sacral spine
The sacral spine is represented by 5 fused vertebrae. They are designated S1-S5. The vertebrae of the department do not fuse immediately. Fusion begins at approximately 14 years of age and is completed by 25 years of age. It is not uncommon for the sacrum to fuse with the 5th lumbar vertebra only after 25 years.
The fused vertebrae are called the sacrum. It looks like a pyramid, pointing downwards.
 The base of the sacrum with its anterior edge forms an angle protruding forward, together with the L5 vertebra. On the base there are 2 articular processes that are directed backward and slightly to the side.
The base of the sacrum with its anterior edge forms an angle protruding forward, together with the L5 vertebra. On the base there are 2 articular processes that are directed backward and slightly to the side.
On the front side of the sacrum there are visible transverse lines - the places of fusion of the vertebrae. Along the edges there are pelvic sacral foramina through which the spinal nerves exit.
The posterior surface of the sacrum is covered with 3 lines of scallops. They are formed by fusion of the rudiments of the articular and spinous processes.
Inside the sacrum there is a continuation of the spinal canal, which ends in the inferior sacral foramen. This hole is important in medicine. This is where the epidural block is performed.
Thanks to this structure of the sacral region, intervertebral hernias practically do not occur in it.
Coccygeal region
This section does not belong to the lumbosacral region, but is the final part of the spine. The coccyx consists of 3-5 vertebrae fused together, which have lost their characteristic features. This department does not perform any important role in the human body. Articular cartilage and adjacent ligaments provide good mobility of the tailbone, so that it can tilt back during childbirth.
Department bends
The lumbar spine has a physiological forward curve called lumbar lordosis. It begins to form in childhood from the moment the child begins to walk upright. Due to the posterior displacement of the load axis in conditions of lumbar bending, circular rotation of the body is ensured.
The sacral section has a curve directed backwards. It is called sacral kyphosis.
These curves are very important for the entire body. Thanks to them, shock-absorbing properties of the spine are ensured, shocks during running and walking are softened, which protects the brain from damage when the body moves.
Ligaments
 The department is strengthened by the following ligaments: posterior longitudinal, supraspinous (absent at the level of the 5th lumbar-1st sacral vertebrae), transverse body, transverse sacral, transverse iliac, sacrotuberous, sacrococcygeal, yellow, etc.
The department is strengthened by the following ligaments: posterior longitudinal, supraspinous (absent at the level of the 5th lumbar-1st sacral vertebrae), transverse body, transverse sacral, transverse iliac, sacrotuberous, sacrococcygeal, yellow, etc.
All ligaments play a very important role, as they fix the spinal column and regulate movements in it. They limit the tilt of the body to the sides, forward and backward, while compensating for displacement of the vertebrae.
Innervation of the department
The lumbar plexus is formed by the interweaving of the I-IV lumbar spinal nerves. It resembles the shape of a triangle with the apex directed along the vertebral bodies. The lumbar plexus branches into terminal and collateral branches. The latter innervate the quadratus lumborum muscle and the psoas major and minor muscles. Terminal branches are represented by the ilioinguinal, iliohypogastric, femorogenital, femoral, obturator nerves and the cutaneous nerve of the thigh.
The sacral plexus is formed by the lumbosacral trunk and the 1st-3rd sacral nerves. It is located under the pelvic fascia on the front of the body of the piriformis muscle. The sacral plexus has 1 terminal and 6 collateral branches, which in turn are divided into many nerves.
DISEASES AND INJURIES
This part of the spine is most often subject to various injuries and pathologies. The reason for this is the peculiarities of the functioning of the department. It is here that there is the greatest freedom of movement of the vertebrae, which need to support the entire mass of the overlying sections.
Also, it is this department that bears the greatest load when lifting and moving heavy objects, during prolonged sitting, when working in a bent position or associated with frequent bending and straightening, etc.
Injuries can occur due to an unsuccessful fall from a height, the collapse of heavy objects (for example, the collapse of a building), as well as due to an accident. Lesions of the spine in this section are very dangerous, as they can cause complete immobility or even death.
Pain in the lumbar and sacral spine can occur not only due to injuries. Its cause may be:

In some cases, lower back pain does not indicate problems with the spine. This is the so-called moving pain in diseases of the internal organs. Therefore, if you experience even mild pain or discomfort in the lower back, you should seek help from a doctor. Based on the tests and studies performed, he differentiates the disease and prescribes appropriate treatment.
Risk factors for the development of diseases of the lumbosacral region:
- congenital anatomical features of the spine;
- previous spinal column injuries;
- overweight;
- high growth;
- smoking;
- poor physical development;
- psychological factors.
Prevention of lower back diseases
To avoid diseases of the lumbosacral region, you should adhere to the following recommendations:
- monitor posture and correct body position during work and rest;
- play sports: yoga, gymnastics, etc.;
- try not to carry weights;
- avoid drafts and hypothermia;
- distribute weights evenly between your hands;
- sleep on an orthopedic mattress;
- monitor your weight;
- get rid of bad habits;
- change body position as often as possible when working in one position for a long time.
Cure arthrosis without drugs? It's possible!
Get the free book “Step-by-step plan for restoring mobility of the knee and hip joints with arthrosis” and start recovering without expensive treatment and surgeries!
Get the book
Without them, none of his movement would have been possible. At the same time, they are used by the human body not only for movements, but also play an important static supporting role, supporting and fixing among themselves both individual elements of the spine - the vertebrae, and the spine as a whole, setting and maintaining its natural curves. Thus, the back muscles do not rest for a minute in an active, awake person in an upright position. One can imagine how tediously hard their work is.
Main functions of the back muscle
Let us systematize the above by listing the main functions performed by the back muscles:
- Permanent fixation of the vertebrae among themselves to provide immovable support. Without this, none of our turns and bends, flexions and extensions would be possible.
- Keeping your back and neck upright
- Ensuring motor activity of all spinal regions
- Maintaining the natural curvature of the back (cervical and lumbar lordosis and thoracic kyphosis) within the required limits
- Cushioning of the spine during active movements leading to shocks, shocks and vibrations
The back muscles are not a homogeneous muscle mass. There are many of them and they come in different sizes, types and functions. They are superficial and deep. Both types consist of two layers.
Let's look at the back muscles from an anatomical perspective and highlight the most important of them.
The most important of them, supporting the spine vertically, is erector muscle (erector):
This is a powerful muscle located on the surface of the deep ones, running along the entire spinal column and filling all the depressions from the spinous processes to the costal surfaces.
All back muscles have their own characteristics, the main ones being:
- Start
- fastening
- functions performed by it
So, the characteristics of the erector dorsi muscle.
Start:
- posterior surface of the sacrum
- posterior iliac crest
- spinous processes of the lower lumbar vertebrae
- thoracolumbar fascia
- lateral - iliocostal
- medially - spinous
- between these two is the longest
All parts have different places fastenings:
- ribs
- transverse and spinous processes
Functions:
- vertical position support
- extension of the spine and its inclinations
- head turns
- partially involved in respiration
On the surface of the back you can see two more of the largest intersecting muscles:
These are the trapezius and latissimus. Their name itself speaks volumes about their external characteristics.
Trapezius muscle:
Two muscle triangles on either side of the spine, with a base near the vertebral axis and an apex near the acromion of the scapula, form a trapezoid shape. Their tendons are short, and only at the border of the cervical and thoracic regions are they slightly longer, forming a diamond-shaped area.
Start:
- spinous processes of the thoracic vertebrae
- nuchal ligament - a thin elastic triangular plate coming from the spinous processes and attached to the occipital crest and protrusion
Fastening:
- Acromial end of the clavicle
- Acromion and scapular axis
Functions:
- Hands up
- Movement of the shoulder blades - raising, lowering, bringing the shoulder blades closer together
- Head tilts in different directions
Latissimus
The latissimus dorsi muscle covers a wide area: from the humerus to the iliacus, crossing the back obliquely, occupying its entire lower part and forming the lumbar triangle below.
Covered at the top in a small area near the trapezoidal spine.

Start:
- spinous processes of the extreme 4 - 6 vertebrae of the thoracic region and all vertebrae of the lumbar and sacral region
- four lower ribs to which muscle teeth are attached
- The thoracolumbar fascia is a membrane that contains the deep muscles of the lumbar and thoracic regions. Attachment occurs by fusion of the smooth tendon area (aponeurosis) of the latissimus muscle with the fascia
- iliac crest
Place of its attachment:
- crest of the lesser tubercle of the humerus
The latissimus dorsi muscle performs the following functions:
- Provides movement of the shoulder with pulling the arm back to the spinal axis with pronation(rotating inward)
- Allows the body to be pulled towards the arm while securing the latter. With its powerful development it becomes possible brachiation- movement with the help of hands, which is always readily used by our relatives - monkeys
Rhomboid major muscle
It is located under the trapezoid and has the shape of a rhombus.
Start
- two outermost cervical vertebrae
- 4 upper pectorals
Fastening
- to the medial edge of the scapula
Functions:
- Attraction of the scapula towards the spine and upward
- Fixation of the medial edge of the scapula to the chest
Big round
The teres major muscle of the back has a flat, elongated shape. The back is covered by the latissimus dorsum, in front - the triceps humerus.
Start:
- inferior angle of the scapula
- fascia of the infraspinatus muscle (filling the fossa of the scapula)
Fastening:
- crest of the tubercle of the humerus with the help of tendons located in the subtendinous bursa
It belongs to the muscles of the upper limb, hence its importance in performing such arm movements:
- pulling the arm down and back
- adduction- bringing the arm to the body
- pronation- inward rotation
The role of the oblique muscle in the functionality of the spine. In the muscles of the lower body you can see another important object, which, although it is an abdominal muscle, in its functions plays a big role for the lower back. This is the oblique abdominal muscle.
There are two types of it:
External oblique
Start:
- outer surface 5 - 12 ribs
Fastening:
- external line of iliac crest
- pubic symphysis
- Linea alba - white collagen fibers located along the midline of the abdominal wall
Internal oblique- this is a wide muscle-tendon plate located under the external muscle
Start:
- intermediate line of the iliac crest
- thoracolumbar fascia
- lateral (side) part of the inguinal ligament
Fastening:
- outer cartilaginous surface of the lower ribs
- linea alba (here the attachment is carried out using a wide tendon)
The external oblique and internal oblique are involved in a number of functions:
- Movements of the chest and pelvis
- Torso rotations
- Spinal flexion
From this it can be seen that not only the muscular system of the back, but also the abdomen plays a large role in the motor function of the spine.
Two weak points in the back. The external oblique and internal oblique muscles are involved in the formation of two important areas of the human body, weakness of which can contribute to the development of a lumbar hernia. These are the so-called:
Lumbar triangle, also called Petit's triangle
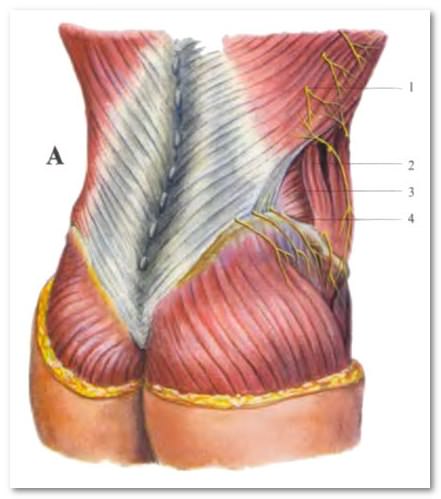
This is a section of the rear wall, limited on three sides:
- behind - latissimus muscle
- in front - external oblique
- below - the iliac crest
The bottom of the triangle is formed by the oblique and transverse abdominal muscles. Essentially, a triangle is a small gap between the edges of the latissimus and external oblique, which does not occur in everyone, but in about 75% of people
Lumbar quadrangle of Grunfeld-Lesgaft
Bounded on four sides:
- superior lateral – 12th rib and serratus inferior muscle
- lateral - external oblique (its posterior edge)
- bottom - edge of the internal oblique
- medial - edge of the sacrospinous
This place is considered weak due to the fact that the oblique abdominal muscles do not cover the quadrangle, so it is not strengthened, and in this place there is a high risk of developing a lumbar hernia.
Taking care of the back muscular system
The anatomy of the back muscles and description of muscle functions show the vital need to strengthen them. Often, incorrect posture, which then leads to many diseases of the spine, occurs due to muscle asymmetry, which can only be eliminated through intensive training. In addition to regular back exercises, special ones are also performed using exercise machines.
To keep your back muscle system in good shape, try to follow three simple rules:
- Be sure to start your day with morning exercises
- Stay less in a relaxed “jelly” position
- Sleep on a hard, flat surface or on a special orthopedic mattress
But it would be wrong to constantly punish our muscles, keeping them in a “black” body and not allowing them to relax even for a minute. So be sure to relax them. Relaxation methods.
The thoracolumbar fascia (THF) is a dense, multi-layered system of connective tissue located in the lower back. It forms a dense fibrous sheath in which the deep muscles of the back lie.
This fascia consists of two layers - deep (anterior) and superficial (posterior).
The deep layer of the thoracolumbar fascia stretches between the transverse processes of the lumbar vertebrae, the iliac crest and the 12th rib. It is present only in the lumbar region and lies in the space between the quadratus lumborum muscle, m. qudratus lumborum, and the erector spinae muscle m. erector spinae.
The superficial layer of the thoracolumbar fascia is attached below to the iliac crests, laterally reaches the corners of the ribs and medially is attached to the spinous processes of all vertebrae, except the cervical ones. It reaches its greatest thickness in the lumbar region, and in the upper sections it becomes significantly thinner. Laterally, along the lateral edge of m. erector spenae, the superficial leaf fuses with the deep one. In this way, a fibrous vagina is formed, in which the lumbar part of the m lies. erectoris spinae; the upper sections of this muscle are located in the osteofibrous sheath of the back.
The latissimus muscles and the posterior inferior serratus muscles begin from the superficial leaf. The transverse abdominal muscle begins from the deep layer of fascia, as well as from the place of its fusion with the superficial layer.
Some muscles influence the configuration and structure of the PGF. The erector spinae muscle creates tension caudally through the fibrous sheath. The latissimus dorsi, trapezius, rhomboids, and serratus muscles exert a strong influence from above. The transverse abdominis muscle exerts a lateral influence; it is obvious that the internal oblique muscles can also influence the thoracolumbar fascia. The lower extremities act through the gluteal fascia, from the iliac crest laterally through the gluteal muscle, and medially from the posterior superior ilium.

Function

The PGF forms a stable, relatively inelastic support, which ensures stabilization of the pelvis, torso and limbs, and also distributes the load between different zones.
When the transverse abdominis muscles are activated to pull the iliacus muscles toward the midline, the mesh structure of the thoracolumbar fascia limits the lateral movement of the pelvic bones and stabilizes the sacroiliac joints.
The horizontal tension created by the transverse abdominis muscles and thoracolumbar fascia effectively compresses the abdominal cavity and stabilizes the pelvis and lumbar spine.
Different muscles contribute to balanced tension in the rhomboid
thoracolumbar fascia, including the erector spinae muscle groups (purple arrows), latissimus dorsi (blue arrows), transverse abdominis (green arrows), and gluteal muscles (white arrows)
Dysfunction
Maintaining proper mobility and stability in the thoracolumbar fascia is critical in preventing injury, pain, and dysfunction of the pelvis and lower back. Deviations in body position, asymmetric muscle tension, and violation of the motor stereotype - all this contributes to distorted and ineffective functioning of the fascial system. Proper identification and elimination of tension in the PMF contributes to normal and effective muscle function.
Exercises to eliminate dysfunction

- Sit on the floor, stretch your legs forward.
- Pull your socks towards you.
- Extend both arms forward, lean forward, and try to touch your stomach to your hips.
- Stay in this position and take a few deep breaths.
This pose helps relieve tension in the psoas, iliacus, rectus femoris, and lower back.
Additionally, this exercise helps restore a neutral position in the pelvis and lumbar spine by increasing vertical height and decreasing horizontal pressure in the thoracolumbar fascia; exercise improves sacroiliac and lumbar stability.
